Will Braces Stop Jaw Popping?
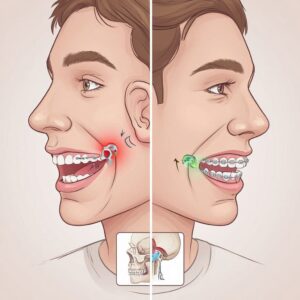
The sound is unmistakable. You yawn after a long meeting or bite into a crusty sandwich, and there it is—a distinct click, pop, or even a grinding sensation right in front of your ear. It doesn’t necessarily hurt every time, but it’s annoying. And sometimes, it’s downright painful. If you are already considering straightening your teeth or fixing an overbite, you might be wondering: Will braces stop jaw popping?
It is a logical question. After all, braces move teeth and change how your upper and lower jaws meet. It stands to reason that changing that alignment might quiet the noise. However, the relationship between orthodontic hardware and the temporomandibular joint (TMJ) is one of the most misunderstood topics in dental health.
The answer is not a simple yes or no. For some people, braces are the exact solution needed to stop the popping permanently. For others, braces might temporarily make the noise worse before it gets better. And for a specific group of patients, braces will have absolutely zero effect on the jaw noise because the source of the problem lies elsewhere.
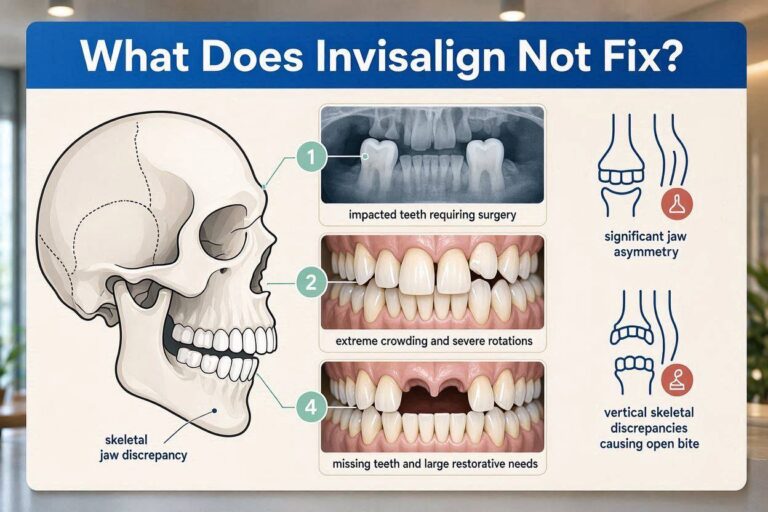
This comprehensive guide will dissect the mechanics of jaw popping, the specific types of bite misalignment that cause it, and how traditional braces or clear aligners (like Invisalign) interact with your jaw joint. We will separate fact from marketing hype and provide you with the realistic, clinical information you need before you schedule that orthodontic consultation.
Understanding the “Pop”: Anatomy of Jaw Noise
Before we can answer whether metal brackets and wires can silence a joint, we need to understand exactly what is making that sound. The human jaw is a marvel of engineering, but it is also a common source of mechanical failure.
The Temporomandibular Joint (TMJ) Basics
You have two temporomandibular joints, one on each side of your face, located just in front of your ears. They connect your lower jaw (mandible) to the temporal bone of your skull. Unlike a simple hinge like your elbow, the TMJ is a “ginglymoarthrodial” joint. That is a fancy way of saying it does two things at once: it rotates like a hinge and slides forward and backward like a drawer.
Between the skull bone and the jawbone sits a small, disc-shaped piece of cartilage. This articular disc acts as a shock absorber and a spacer. It is attached to the jawbone by ligaments and moves in sync with the jaw as you open and close.
The Source of the Pop: Disc Displacement
That clicking or popping sound is almost always the sound of this articular disc snapping out of place and then snapping back into place (or snapping over a bony obstacle).
Here is the mechanical sequence of a typical “reciprocal click” (pop on opening and closing):
-
Mouth Closed: The disc sits snugly between the condyle (the round top of the jawbone) and the skull socket.
-
Opening Begins: Due to muscle tightness, scar tissue, or a deep overbite, the condyle pulls forward but the disc gets “stuck” behind it.
-
The Pop: As you open wider, the pressure builds until the condyle suddenly jumps over the back edge of the disc and onto the middle of the disc. That jump is the pop you hear.
-
Closing: As you close, the condyle slides backward off the disc, creating a second, often softer, click.
Important Note: Painless Clicking vs. Painful Locking
This is a crucial distinction that every reader must understand.
-
Painless Clicking (Reducing Disc Displacement): The disc slips off but slips back on. The joint functions, just with a soundtrack. Many people live with this for decades without ever needing treatment.
-
Painful Clicking/Catching: The disc is pinching the highly innervated tissue behind it (the retrodiscal tissue). This often leads to inflammation and soreness.
-
Locking (Non-Reducing Disc Displacement): The disc slips off and stays off. The jaw cannot open fully (closed lock) or cannot close fully (open lock). This is a medical emergency in the dental world.
Where do braces fit in? Braces are primarily a tool for addressing the bony and tooth environment. They can change the position of the condyle within the socket, which in turn can allow the disc to find a more stable position. They do not, however, directly repair a torn ligament or reshape a deformed disc.
Will Braces Stop Jaw Popping? The Three Scenarios
Let’s get directly to the core question with absolute clarity. Orthodontic treatment falls into three distinct categories regarding jaw joint noise.
Scenario 1: Yes, Braces Can Completely Resolve the Popping
This is the ideal outcome and it happens more often than skeptics admit, provided the diagnosis is correct. Braces stop jaw popping in this scenario because the popping was caused by malocclusion-induced instability.
How Malocclusion Causes Jaw Popping:
Imagine a door that doesn’t hang square on its hinges. Every time you close it, you have to lift the handle up and force it into the frame. Over time, the hinges creak and the latch mechanism pops loudly. Your jaw is the same. If your teeth don’t fit together in a stable, balanced way, your jaw muscles have to contort the condyle into an unnatural position to achieve a bite.
The most common bite issues that cause this “mechanical derangement” include:
-
Deep Overbite (The Most Common Culprit): When the upper front teeth completely cover the lower front teeth, they act like a ramp. They force the lower jaw backward into the ear canal. This backward position crushes the retrodiscal tissue and forces the disc forward off the condyle. When you open, it pops.
-
Crossbite (Unilateral): If the back teeth on the right side bite inside the lower teeth but the left side bites normally, the jaw must shift sideways to chew. This lateral shift torques one TMJ and stretches the other. Popping occurs on the side being forced out of alignment.
-
Open Bite (Anterior): When the front teeth don’t touch, all the chewing force is concentrated on the back molars. This overloads the joint and can cause ligament laxity (looseness) leading to disc slippage.
The Mechanism of Relief:
When braces level the teeth and correct the overbite or crossbite, the muscles can relax. The condyle is no longer being forced backward or sideways by the teeth. It settles into a “centric relation”—the orthopedic sweet spot where the disc has the most room to function.
| Clinical Outcome | Before Braces | After Braces (Stable Bite) |
|---|---|---|
| Condyle Position | Forced posterior (backward) | Centered in the fossa (socket) |
| Disc Position | Anterior displacement (slipped forward) | Recaptured or compensated |
| Muscle Activity | Hyperactive to avoid pop | Normalized tone |
| Joint Sound | Loud, audible pop | Silent or soft click |
Clinical Quote: “In my practice, patients with Class II deep bites are the most likely to report a complete cessation of TMJ clicking after comprehensive orthodontic treatment. We aren’t treating the disc; we are fixing the environment the disc lives in.” — Dr. James R., Orthodontist (paraphrased clinical experience).
Scenario 2: No, Braces Will Not Stop the Popping
It is vital to be honest about this limitation. Braces are not a cure-all for TMJ disorders (TMD). In fact, using braces to “treat” a popping jaw when the cause is not orthodontic can be an expensive and frustrating waste of time.
When Braces Are Ineffective for Jaw Popping:
-
Osteoarthritis (Degenerative Joint Disease): This is “wear and tear” arthritis. The smooth surface of the condyle or socket has become rough like sandpaper. The pop is crepitus (a grinding, gravelly sound). Braces cannot regrow smooth cartilage. Straightening teeth will not silence the grinding of bone on bone.
-
Rheumatoid Arthritis: An autoimmune condition attacking the joint lining. This requires medical management with a rheumatologist, not an orthodontist.
-
Chronic Bruxism (Nighttime Grinding/Clenching): This is the #1 reason braces fail to stop popping. You can have perfect teeth alignment, but if you clench your jaw with 900 pounds of force while you sleep, you are squeezing the disc like a grape. The disc will slip out regardless of how straight your teeth are. Braces do not change your subconscious stress response.
-
Ligament Hyperlaxity: Some people, particularly those with Ehlers-Danlos Syndrome or general joint hypermobility, have ligaments that are too stretchy. The disc floats around like a raft in a storm. Braces cannot tighten ligaments.
-
Macro-Trauma: A direct blow to the jaw (car accident, sports injury) that tore the attachment of the disc. This is a structural tear. Braces move teeth; they do not suture torn cartilage.
The Warning About Invisalign and Clenching:
This is a critical nuance. Some patients seek Invisalign for a popping jaw, only to find the popping gets worse during treatment. Why? Because wearing plastic aligners 22 hours a day often triggers a subconscious clenching reflex. The plastic provides a smooth, satisfying surface to grind on. This increased muscle activity can inflame the joint and increase disc displacement. A skilled orthodontist will screen for bruxism before starting clear aligner therapy.
Scenario 3: Temporary Increase in Popping (The Adjustment Phase)
This is perhaps the most alarming scenario for patients, but it is often a normal part of the journey. You get braces put on, and within two weeks, your jaw is popping more than it ever did before.
Why does this happen?
You have just glued foreign objects to your teeth. Your bite height has changed by fractions of a millimeter. Your tongue doesn’t know where to rest. The muscles of mastication (chewing) are in a state of proprioceptive confusion. They are searching for a stable bite that no longer exists because the teeth are moving.
During this phase (usually weeks 1 through 8 of treatment), the muscles might spasm and pull the disc off track more frequently.
How to distinguish “Bad” Popping from “Adjustment” Popping:
| Feature | Adjustment Popping (Benign) | Pathological Popping (Red Flag) |
|---|---|---|
| Pain Level | None or very mild soreness | Sharp, electric, or radiating ear pain |
| Range of Motion | Normal opening (35-45mm) | Restricted opening (can’t fit 3 fingers) |
| Timing | Intermittent, changes day-to-day | Constant, every time you open |
| Locking | Never locks | Jaw catches open or closed |
Important Note for Brace Wearers: Never stop wearing your elastics (rubber bands) because of jaw popping without consulting your orthodontist. The elastics are often specifically designed to seat the condyle in the correct position. Removing them can allow the jaw to drift into a more unstable, louder popping position.
The Diagnostic Path: Before You Get Braces
If your primary concern is jaw popping and you want to know if braces are the right tool, you cannot skip the diagnostic phase. Walking into an orthodontist and saying “I want braces to fix my TMJ” is like walking into a mechanic and saying “I want new tires to fix my check engine light.” It might help, or it might be a $7,000 guess.
The Clinical Exam: What a Specialist Looks For
A dentist or orthodontist trained in TMD (or a TMJ specialist) will perform specific tests before taking impressions for braces.
-
The Load Test: The doctor will place cotton rolls or a leaf gauge between your back teeth and have you close gently for 5 minutes. This deprograms the muscles. If the popping stops or significantly reduces when the bite is opened this way, it is a strong indicator that braces (which can change the bite height) will help.
-
Palpation of the Lateral Pterygoid: This is the muscle that pulls the disc forward. If this muscle is rock hard and tender, the popping is muscular in origin. Braces change the hard tissue; they may not change this muscle’s habits.
-
Range of Motion Measurement: Can you open 40mm? Is there deviation? A jaw that deviates to one side then pops signals a disc obstruction on that side.
Imaging: Seeing the Unseen
This is non-negotiable for complex cases. A standard Panoramic X-ray (the one that spins around your head) is useless for seeing the TMJ disc.
-
Cone Beam CT (CBCT): This shows the bone. It reveals flattening of the condyle, bone spurs (osteophytes), or arthritis. If the bone is damaged, braces will not fix the pop.
-
MRI (Magnetic Resonance Imaging): This is the Gold Standard for seeing the disc. It shows exactly where the disc is relative to the condyle and whether it is reducing (popping back) or stuck.
Critical Reality Check: Most standard orthodontic consultations for cosmetic braces do NOT include a CBCT of the TMJ or an MRI. They include photos of your smile and a panorex of your tooth roots. If jaw popping is your primary concern, you must advocate for a deeper level of imaging or seek a second opinion from a dentist with a focus on Neuromuscular Dentistry or Orofacial Pain.
Braces vs. Other Treatments for Jaw Popping
Since we are exploring whether braces stop jaw popping, we must compare them against the established standard of care for TMJ disorders. Braces are a long-term structural solution. Other treatments are often short-term symptomatic relief.
Comparison Table: Braces vs. Common TMD Therapies
| Treatment Modality | Mechanism of Action | Effectiveness for Popping | Cost & Duration | Best For |
|---|---|---|---|---|
| Braces / Invisalign | Repositions teeth to create orthopedic stability for the condyle. | High (if malocclusion is cause) | $5,000 – $8,000+ / 12-24 months | Deep bite, crossbite, missing teeth shifting bite. |
| Night Guard (Splint) | Provides a smooth plastic barrier to absorb clenching force; prevents tooth wear. | Moderate (prevents morning lock, reduces muscle tension) | $500 – $1,500 / Indefinite wear | Bruxism (grinding), mild muscle spasm. |
| Anterior Repositioning Splint | A special guard that forces the lower jaw forward to recapture the disc. | High (Temporary) | $2,000 – $4,000 / 3-6 months | Acute disc displacement with locking. |
| Physical Therapy | Exercises to strengthen jaw stabilizers, manual therapy to stretch tight muscles. | Moderate to High | $100+ per session / 6-8 weeks | Muscular TMD, postural issues (forward head posture). |
| Arthrocentesis / Surgery | Flushing the joint with fluid to remove inflammation debris. | High (for mechanical block) | $2,000+ / Procedure | Persistent locking, arthritis debris. |
The Splint Question: A Necessary Detour?
Many readers will encounter a significant fork in the road. They want braces to stop the popping, but the dentist says: “First, we need to stabilize your joint with a splint for 6 months.”
Is this necessary or a scam?
It is often 100% necessary.
The Analogy: You have a sprained ankle (inflamed TMJ) and you also need new running shoes (braces). If you put the new shoes on and go run a marathon immediately, you will destroy your ankle further.
The Rationale:
-
Phase I (Splint Therapy): The splint deprograms the muscles and allows the inflamed joint to heal. It lets the doctor find the true stable position of your jaw without the teeth getting in the way.
-
Phase II (Braces/Orthodontics): Once the joint is quiet and the popping is reduced, the orthodontist moves the teeth to meet the jaw in that new, healthy position.
Skipping Phase I and going straight to braces on an inflamed joint can result in a condition called “Orthodontic TMD” — you finish braces with straight teeth but a jaw that is in constant, permanent spasm.
In-Depth: Specific Bite Problems and Jaw Popping Outcomes
Let’s dive deeper into the specific orthodontic problems that are most likely linked to that annoying click. Understanding your specific malocclusion category gives you the most accurate prediction of whether braces will stop the jaw popping.
1. The Deep Bite (Overbite) Connection
How it Causes Popping:
A deep bite is when the upper front incisors vertically overlap the lower incisors by more than 3-4mm. In severe cases, the lower teeth bite into the roof of the mouth (palate).
This creates a distalizing force. Every time you close your mouth, your chin is forced backward toward your throat. This pushes the condyle against the back wall of the socket, directly into the bilaminar zone—a highly vascular, highly innervated tissue that is not designed to bear weight.
The Sound:
The pop in deep bite patients is usually a single, loud clunk about halfway through opening. It occurs because the condyle is trapped behind the disc and has to “jump” over the back lip of the disc to get onto the articular surface.
Will Braces Stop Jaw Popping Here?
Likelihood: Very High.
Treatment Nuance:
Fixing a deep bite with braces usually requires bite turbos (little blue or tooth-colored bumps glued to the back of the front teeth) or bite ramps on clear aligners. These props prevent you from closing all the way down.
-
Immediate Effect: Patients often report immediate relief of popping while wearing the braces. Why? Because the turbos prevent the jaw from fully seating into that damaging backward position. The joint gets a 12-month vacation while the teeth move.
Patient Story Context: *A 29-year-old female presented with chronic right TMJ clicking and weekly tension headaches. She had a 90% deep bite. Within one month of braces placement with posterior bite turbos, the clicking reduced by 80%. By the end of 18 months of treatment, the click was absent and the jaw opening path was straight.*
2. The Posterior Crossbite and Facial Asymmetry
How it Causes Popping:
A crossbite is a mismatch in the width of the upper and lower jaws. In a unilateral crossbite (one side only), the upper teeth are too narrow and bite inside the lower teeth on the affected side.
To get the teeth together to chew, the patient must shift their lower jaw sideways every single time they close.
The Consequences of a Lateral Shift:
-
The TMJ on the shifted side gets compressed. The disc gets squeezed out of place.
-
The TMJ on the opposite side gets stretched. The ligaments become loose.
-
The muscles on one side of the face become hypertrophic (larger), leading to facial asymmetry.
The Sound:
The pop here is often a “reciprocal click” that is louder on the side of the shift.
Will Braces Stop Jaw Popping Here?
Likelihood: High, provided expansion is achieved.
Treatment Nuance:
This often requires more than just braces on the teeth. It may require a Palatal Expander (for children/teens) or Surgically Assisted Rapid Palatal Expansion (SARPE) (for adults) to widen the upper jaw bone. If the bone is too narrow, braces alone just tip the teeth and the jaw shift (and the pop) will return as soon as braces are removed.
3. The Anterior Open Bite
How it Causes Popping:
An anterior open bite is a gap between the upper and lower front teeth when the back teeth are touching. This is common in thumb suckers, tongue thrusters, and patients with degenerative joint disease (where the condyle bone actually dissolves, making the chin rotate backward and down).
The Mechanism:
Because the front teeth cannot cut food or provide a “stop” for closure, all the force of chewing is placed on the last two molars. These molars act like a fulcrum. The heavy chewing load pounds the TMJ into the socket, wearing down the disc and bone.
Will Braces Stop Jaw Popping Here?
Likelihood: Moderate to Low (Depends on Etiology).
This is where we must be extremely careful.
-
If caused by Tongue Thrust: Braces can close the space, but if you don’t fix the tongue thrust (with Myofunctional Therapy), the open bite will return and the popping will return. The tongue is stronger than braces.
-
If caused by Condylar Resorption: This is an active arthritic condition where the jawbone is melting away. Do NOT get braces first. Braces can mask the problem while the joint silently destroys itself. An MRI is mandatory here.
The Clear Aligner (Invisalign) Dilemma
A significant portion of the adult population seeking to stop jaw popping wants to avoid traditional metal braces. They ask specifically about Invisalign or other clear aligners.
The answer is nuanced. Will braces stop jaw popping? Yes, often. Will clear aligners stop jaw popping? Sometimes, but with added risks.
The Advantages of Aligners for TMJ
-
Posterior Open Bite Creation: Aligners cover the back teeth. This creates a temporary space (a “disclusion”) between the molars when the aligners are in. This is therapeutic. It unloads the TMJ for 20+ hours a day, reducing inflammation and popping just like a splint would.
-
Slow, Controlled Movements: Aligners move teeth more slowly than traditional braces (in some protocols). This can be gentler on a sensitive joint.
The Disadvantages of Aligners for TMJ
-
The Clenching Phenomenon: This is the elephant in the room. Studies show that up to 50-60% of Invisalign patients report increased clenching or grinding during treatment. The plastic acts as a perfectly fitted night guard, which can be a “chew toy” for a subconscious bruxer. This increased muscle load can displace the disc.
-
Lack of Rigid Archwire Support: Traditional braces are connected by a stiff metal wire. This wire acts as a splint for the jaw. If the muscles spasm, the wire helps hold the teeth and jaw in alignment. Aligners are plastic. They can be bitten through or can flex under heavy clenching force, offering less orthopedic support.
-
Vertical Control Difficulty: Intruding (pushing up) over-erupted front teeth in a deep bite is sometimes harder with aligners than with braces. Since deep bite is a primary cause of popping, this is a critical limitation.
Decision Checklist for Aligners with a Popping Jaw
If you are leaning toward clear aligners but have jaw popping, ask these questions first:
-
Do I clench my teeth when stressed or driving? (If yes, you are a high-risk aligner patient).
-
Do I wake up with a sore jaw? (Indicator of sleep bruxism).
-
Does my orthodontist have experience treating TMD patients with aligners? (Not all do).
-
Will my treatment plan include “bite ramps” behind the front teeth? (These are crucial for deep bite/TMJ cases).
Managing Jaw Popping During Orthodontic Treatment
Let’s assume you’ve started treatment. The braces are on or you are on Tray 3 of 30. The jaw is popping. How do you manage the next 18 months without going crazy?
Immediate Self-Care Strategies (The R.I.C.E. for Jaw)
-
Soft Diet Discipline: This is the single most effective behavioral change. For the first 6 weeks of braces (and any flare-up period), avoid:
-
Chewy bread (bagels, pizza crust).
-
Raw carrots and apples (cut them into tiny pieces).
-
Chewing gum (absolute poison for a popping TMJ).
-
Steak or tough meats.
-
-
The “N” Resting Position: Your teeth should NEVER be touching when you are not eating. Train yourself. Lips together, teeth apart. Say the letter “N” and hold your tongue on the roof of your mouth. This is the physiologic rest position.
-
Heat Therapy: Apply a moist heating pad to the side of the face for 15 minutes before bed. This increases blood flow to the lateral pterygoid muscle, helping it relax so the disc can seat better overnight.
When to Call Your Orthodontist Immediately
Do not wait for your next 8-week adjustment appointment if you experience:
-
Locked Jaw: You cannot open your mouth wider than 20-25mm (about the width of two fingers). This means the disc is not reducing. Early intervention with muscle relaxants or manipulation is key.
-
Acute Change in Bite: Suddenly, only ONE tooth is touching on one side when you close. This can indicate significant joint inflammation/swelling that has shifted the condyle position.
-
Severe Ear Pain: While some “ear stuffiness” is normal with braces, sharp, stabbing ear pain that is not an infection warrants a check of the TMJ.
Life After Braces: Retention and Long-Term Joint Health
Congratulations, the braces are off! Your teeth are straight. But the journey to a quiet jaw isn’t over. In fact, the retention phase is where many success stories unravel.
Why Popping Returns After Braces
This is a heartbreaking scenario. A patient endures 24 months of braces, enjoys 6 months of a silent jaw, and then 2 years later… pop… it’s back.
Common Culprits for Relapse:
-
Wisdom Teeth Eruption: This is a massive but often overlooked factor. If you are in your late teens or early twenties and your third molars (wisdom teeth) are trying to come in, they can cause anterior crowding. The shifting of the entire arch destabilizes the bite and forces the jaw back into a bad position.
-
Non-Compliance with Retainers: If you don’t wear your retainers, teeth drift. Even a 0.5mm shift in a back tooth can change how the jaw closes and trigger the pop.
-
Unresolved Bruxism: If you never addressed the nighttime clenching, the joint was just taking a vacation during braces. Once the braces are off and you’re back in a hard plastic retainer (which, unlike aligners, does not cover the biting surfaces of the teeth), you can clench down hard, squeezing the joint again.
The Role of the Permanent Retainer
A bonded wire retainer glued to the back of the front 6 teeth is excellent for keeping those teeth straight. However, it does NOT maintain the position of the back molars. Posterior teeth can still drift. This is why a removable retainer (Essix or Hawley) worn at night is non-negotiable for maintaining the orthopedic correction that stopped the popping.
The Long-Term Prognosis: Maintenance is Key
Think of your TMJ like a knee that has had surgery. It’s better, but it’s never “brand new.” You have to manage it.
| Long-Term Habit | Impact on TMJ Popping |
|---|---|
| Nighttime Retainer Wear | Maintains arch form; prevents bite collapse. Essential. |
| Regular Dental Checkups | Catches failing fillings or crowns that change bite height. |
| Stress Management | Reduces diurnal (daytime) clenching. |
| Posture Correction | Forward head posture adds 30+ lbs of strain to jaw muscles. |
Comparative Analysis: Traditional Braces vs. Other Orthodontic Appliances
We’ve discussed braces at length, but what about other gadgets? Patients often get confused by the array of options marketed for TMJ pain.
| Appliance Type | Appearance | Primary Goal | Effect on Jaw Popping |
|---|---|---|---|
| Traditional Braces | Metal/Ceramic brackets | Tooth alignment & Bite correction | Permanent Correction (if malocclusion cause) |
| NTI-tss Device | Small plastic on front teeth | Prevent back tooth contact | Temporary Relief (Reduces clenching intensity, does NOT fix bite) |
| Anterior Growth Guidance Appliance (AGGA) | Metal frame behind teeth | Attempt to remodel upper jaw bone in adults | Controversial & High Risk. Often makes popping worse due to flaring teeth and creating open bites. AVOID for TMD. |
| Twin Block Appliance | Two removable plates (upper/lower) | Posture lower jaw forward in growing kids | Excellent for Popping in Class II kids. Helps the joint remodel naturally. |
Warning on “TMJ Cure” Gadgets: The internet is flooded with “jaw exercisers” or chewing devices that claim to stop popping. Be extremely skeptical. Forcing a joint with a displaced disc to chew on a hard object is like running on a torn meniscus. You risk converting a painless pop into a painful lock.
The Psychological Impact of Jaw Popping and Treatment
This is an aspect of the condition that rarely makes it into clinical brochures but is profoundly important. Living with a jaw that clicks or pops is not just a physical nuisance; it is a psychological burden.
The Anxiety of the Pop
Imagine you are in a quiet room—a library, a meditation class, or worse, leaning in for a first kiss. You open your mouth and CRACK. The sound feels, to you, like a gunshot. You become hyper-aware. You start eating in specific ways, chewing only on the “quiet” side. You avoid laughing too widely. This is called avoidance behavior.
Will braces stop jaw popping? For many, the answer is a resounding yes. But the relief extends far beyond the silence. It restores a sense of normalcy and confidence. Patients report:
-
Improved sleep quality (no more waking up with jaw fatigue).
-
Better concentration (no more constant focus on “not clicking”).
-
Enhanced social comfort.
Coping with the “Braces Worsening” Phase
As we noted earlier, the first few weeks of braces can be loud. The popping might get worse. This can trigger significant anxiety. “I spent all this money to fix it and I broke it worse!”
This is where patient education is critical. Your orthodontist should prepare you for the Proprioceptive Adaptation Period.
Coping Mechanisms:
-
Journaling: Keep a “Jaw Log.” Note the days the popping is loud vs. quiet. You will likely see a pattern: Loud pop on days after eating chewy food, quiet pop on days you ate soup. This gives you a sense of control.
-
Noise Acceptance: Remind yourself: “This is the sound of my joint finding its new home.” It is a mechanical adjustment, not a sign of damage.
-
Soft Earplugs: If the internal noise of the popping drives you crazy while trying to sleep, wearing a soft earplug in the affected ear can dampen the bone-conducted sound.
The Role of Nutrition and Inflammation
While braces change the structure, what you eat changes the environment inside the joint capsule. Inflammation is the enemy of a quiet joint.
Dietary Considerations for the Popping Jaw
If you are undergoing orthodontic treatment specifically to address TMJ popping, adopting an anti-inflammatory diet can accelerate the quieting of the joint.
Foods to Embrace:
-
Omega-3 Fatty Acids: Found in salmon, mackerel, walnuts, and flaxseed. These oils lubricate the joints from the inside out.
-
Magnesium-Rich Foods: Dark leafy greens, almonds, avocados. Magnesium is a natural muscle relaxant. Tight lateral pterygoid muscles pull the disc out of place; magnesium helps them let go.
-
Bone Broth: Contains collagen and glucosamine which support cartilage health (though the disc is dense fibrocartilage, not bone).
Foods to Strictly Avoid (Especially in Month 1 of Braces):
-
Hard, Crunchy Snacks: Chips, pretzels, popcorn. The jarring motion of biting into a chip with new braces causes micro-trauma to the TMJ ligaments.
-
Excessive Caffeine: Caffeine is a vasoconstrictor and a muscle stimulant. It tightens the jaw muscles.
-
Chewing Gum (Even Sugar-Free): We will repeat this until it is ingrained. Never chew gum. The repetitive motion is the worst possible exercise for a displaced disc.
Will Braces Stop Jaw Popping? The Surgical Edge Cases
This guide would be incomplete and frankly dishonest if we did not address the severe end of the spectrum. There are cases where the joint is so damaged that braces cannot stop the popping because there is no disc left to pop.
Anterior Disc Displacement Without Reduction (Closed Lock)
The Scenario: You woke up one morning and could barely open your mouth. You can fit one finger between your teeth. The popping has stopped. This is not good news. It means the disc is stuck in front of the condyle and is acting as a doorstop.
Can Braces Fix This?
No. If the jaw is locked closed, you cannot open wide enough to brush your back teeth properly, let alone undergo 18 months of orthodontic adjustments. This requires immediate medical intervention.
The Pathway:
-
Arthrocentesis: A needle flushes out the inflamed joint fluid. This often releases the “suction cup” effect holding the disc out of place.
-
Manual Manipulation: Under sedation, the doctor pulls the jaw down and forward to “walk” the disc back onto the condyle.
-
Arthroscopy: A tiny camera and instruments are inserted into the joint to cut adhesions (scar tissue).
Where Braces Fit In:
Post-Operatively. After the joint is unlocked and the disc is recaptured, braces are absolutely necessary in many cases. Why? Because the locked position often causes a posterior open bite on the affected side. The teeth no longer touch properly. Braces are used to close that space and provide a stable bite so the disc does not slip off again.
Condylar Resorption (Idiopathic Condylar Resorption – ICR)
This is a condition primarily affecting teenage and young adult females. The condyle (the head of the jawbone) literally dissolves. It is an active, degenerative process.
The Sound:
Crepitus. Grinding. Gritty. Not a clean pop.
Can Braces Stop Jaw Popping Here?
Braces are CONTRAINDICATED. If you put braces on a jaw that is actively dissolving, the orthodontic forces can accelerate the bone loss. You will end up with a severe open bite and a recessed chin.
The Correct Path:
Stabilization via splint therapy for 2+ years to ensure the disease is “burned out.” Then, Orthognathic Surgery (Jaw Surgery) combined with braces. The braces prepare the teeth, the surgeon repositions the jaws, and the joint is stabilized by changing the entire skeletal structure.
The Financial Perspective: Is It Worth the Investment?
Orthodontic treatment is a significant financial undertaking. If your primary motivation is cosmetic straightening, the improvement in jaw popping is a wonderful bonus. But what if your teeth are already straight but your jaw pops constantly? Is $6,000 worth it just to stop a sound?
Cost-Benefit Analysis for “Silence”
| Expense | Estimated Cost (USD) | Longevity |
|---|---|---|
| Comprehensive Braces | $5,500 – $8,000 | Permanent (with retention) |
| TMJ Splint Therapy | $2,500 – $4,000 | 3-5 years (splints wear out) |
| Physical Therapy (12 sessions) | $1,200 – $2,400 | Requires ongoing home exercises |
| Ignoring the Pop | $0 | Potential for future lock, chipped teeth, chronic headaches |
The Hidden Cost of Doing Nothing:
A popping jaw is a pre-arthritic sign. The disc is meant to be a cushion. When it’s out of place, you are rubbing the condyle against the innervated retrodiscal tissue. Over 10-20 years, this tissue perforates. Once there is a hole in the tissue, you have bone-on-bone contact. This is osteoarthritis.
Repairing a perforated disc requires open-joint surgery (arthroplasty). The cost of TMJ surgery far exceeds the cost of braces. Preventative orthodontics is a cost-saving measure in the long run.
Finding the Right Provider: Not All Orthodontists Are Created Equal
If you search “Will braces stop jaw popping?” on Google, you will find thousands of orthodontic websites that say “Yes! We treat TMJ!” It is crucial to vet these claims.
Questions to Ask During Your Consultation
Do not be shy. You are interviewing the doctor for a job that costs thousands of dollars and affects your quality of life.
-
“What percentage of your practice is dedicated to TMD or airway-focused orthodontics?”
-
Ideal Answer: “About 30-40% of my patients have some TMD component.”
-
Red Flag: “Oh, we just straighten teeth.” (This doctor may ignore your popping complaints once the braces are on).
-
-
“Do you take a Cone Beam CT (CBCT) scan for patients with popping?”
-
Ideal Answer: “Yes, we need to see the condylar position and shape.”
-
Red Flag: “We just take a panoramic x-ray.” (This is insufficient for joint diagnosis).
-
-
“What is your protocol if my jaw locks during treatment?”
-
Ideal Answer: “We have emergency slots, we will remove archwires if needed, and we work with a local oral surgeon if necessary.”
-
Red Flag: “Just take ibuprofen and it will be fine.”
-
The Multidisciplinary Team
The best outcomes for complex TMJ popping occur when multiple specialists communicate.
-
Orthodontist: Moves the teeth.
-
Oral Surgeon: Manages the joint/surgery.
-
Physical Therapist: Re-trains the muscles.
-
Myofunctional Therapist: Re-trains the tongue.
If your orthodontist works in a silo and never refers out, you might not be getting the most comprehensive care.
Technology and Innovations in TMJ Orthodontics
The field is advancing rapidly. The days of “just put braces on and hope the jaw quiets down” are fading, replaced by data-driven, 3D-printed precision.
Digital Smile Design and Jaw Tracking
Modern orthodontic software (like the iTero scanner or Primescan) can now map the movement of the jaw. This is called 4D Jaw Motion Tracking.
-
How it Works: A wand tracks your lower jaw as you open and close. The software creates a slow-motion video of your jaw’s path.
-
Benefit for Popping: The software can pinpoint the exact millimeter where the pop occurs. The orthodontist can then design braces or aligners to avoid that specific position, guiding the teeth into a pop-free zone.
TADs (Temporary Anchorage Devices)
These are tiny titanium screws placed in the gum/bone. They are game-changers for popping jaws.
Scenario: A patient has a deep bite causing the jaw to pop backward.
Old Way: Wear headgear (uncomfortable, compliance-dependent).
New Way (TADs): Place two tiny screws in the upper back jaw. Attach elastics from the screws to the front teeth. This intrudes (pushes up) the front teeth without moving the back teeth. The deep bite opens, the jaw pops forward to a relaxed position, and the popping stops without forcing the jaw backward.
TADs allow for “skeletal” correction rather than just “dental” camouflage. This is a more stable, long-term solution for stopping jaw noise.
The Pediatric Perspective: Stopping Popping Early
If you are a parent reading this and you notice your child’s jaw clicking when they eat or yawn, do not wait for all the baby teeth to fall out. This is a critical window of opportunity.
Growing Pains vs. True Pathology
It is true that children’s joints are looser and can be “clicky.” However, a consistent reciprocal click in a child aged 7-10 is often the first sign of a developing skeletal discrepancy (like a narrow upper jaw or a lower jaw that is too far back).
Early Orthodontic Intervention (Phase I)
-
Goal: Guide the growth of the jaws.
-
Methods: Palatal expanders, twin block appliances, reverse pull headgear.
-
Impact on Popping: Profound. By widening the upper jaw or advancing the lower jaw while the child is still growing, you change the anatomy of the joint socket itself. This can permanently silence a popping joint for life.
The Cost of Waiting:
If you wait until age 14-16 (Phase II braces), the bones have fused. You cannot grow the jaw wider without surgery. You can only align the teeth. The structural problem causing the pop remains.
Important Note for Parents: If your child has Sleep Disordered Breathing (snoring, mouth breathing, bedwetting) AND jaw popping, there is a 90% chance the two are connected. The narrow jaw that causes popping also crowds the airway. Early expansion is life-changing for both sleep and jaw health.
The Link Between Posture and Popping
You cannot have a quiet jaw on a crooked neck. This is a biomechanical law.
The Cervical-Cranial-Mandibular Connection
Your head weighs about 10-12 pounds (the weight of a bowling ball). When your head is perfectly balanced over your shoulders, your jaw muscles use about 5% of their maximum force to keep your mouth closed.
The Problem: Forward Head Posture (Text Neck)
Looking down at your phone or hunching over a laptop moves the center of gravity forward. For every inch your head moves forward, the effective weight on your neck and jaw muscles doubles.
To keep your mouth closed against this forward-pulling weight, the muscles under your chin (suprahyoids) and the muscles pulling your jaw back (temporalis) go into a tug-of-war. This tension squeezes the TMJ disc out of place.
Exercises to Complement Braces
While braces fix the teeth, these exercises fix the posture that may have caused the problem in the first place.
-
Chin Tucks (The “Nerd Neck” Fix):
-
Stand against a wall.
-
Pull your chin straight back (like making a double chin).
-
Do NOT tilt your head down.
-
Hold for 5 seconds. Repeat 10 times, 3x per day.
-
Effect: Realigns cervical spine, reduces TMJ load.
-
-
The “Goldfish” Exercise (Partial Opening):
-
Place your tongue on the roof of your mouth.
-
Place one finger on the TMJ in front of your ear.
-
Open your mouth only halfway (before the pop happens).
-
Close slowly.
-
Repeat 10 times.
-
Effect: Strengthens the muscles that pull the disc back onto the condyle.
-
Will Braces Stop Jaw Popping? The Final Verdict Table
To consolidate everything we’ve discussed, use this reference guide to assess your specific situation.
| If Your Situation Is… | Will Braces Likely Stop the Popping? | Additional Steps Required |
|---|---|---|
| Deep Overbite + Popping | YES – Highly Likely | Bite Turbos, possible TADs for intrusion. |
| Crossbite + Lateral Jaw Shift | YES – Likely | Possible Palatal Expansion (especially in kids). |
| Straight Teeth + Nighttime Grinding | NO – Unlikely | Night Guard, Stress Management, Botox for masseter. |
| Jaw Locked Shut (Cannot Open) | NO – Emergency | See Oral Surgeon for Arthrocentesis FIRST. |
| Open Bite + Popping + Receding Chin | CAUTION – Maybe Not | Rule out Condylar Resorption (ICR) via MRI. |
| Arthritis / Crepitus (Grinding Sound) | NO | Braces cannot regrow cartilage. |
| Popping Started After Braces Removed | Relapse | Evaluate Retainer Wear, Wisdom Teeth, Bruxism. |
Conclusion
Will braces stop jaw popping? The answer is a confident yes, but only when the popping stems from a misaligned bite, such as a deep overbite or crossbite. Orthodontic treatment effectively restores the jaw joint’s proper seating by eliminating the dental interferences that force the condyle out of position. However, braces are not a cure-all; if the noise originates from arthritis, ligament damage, or chronic nighttime grinding, braces alone will not silence the joint. Ultimately, achieving lasting relief requires a precise diagnosis, a realistic understanding of the adjustment period, and a commitment to long-term retention to maintain the new, stable joint environment.
Frequently Asked Questions (FAQ)
Q: Can braces cause TMJ or jaw popping if I didn’t have it before?
A: It is rare but possible. This usually happens if the orthodontist moves teeth in a way that creates a new interference in the bite (a “premature contact”) or if the patient develops a clenching habit while wearing aligners. A properly planned case should minimize this risk.
Q: How long after getting braces will the popping stop?
A: It varies. Some deep bite patients notice immediate relief within 1-2 weeks due to bite turbos opening the bite. Others may experience a gradual quieting over 3-6 months as the teeth align and muscles relax. A temporary increase in popping during the first 8 weeks is common and normal.
Q: Is Invisalign better than braces for jaw popping?
A: It depends on the patient. Invisalign is excellent for creating a “splint effect” that unloads the joint. However, if you are a clencher, Invisalign can increase muscle activity and popping. Metal braces offer more rigid jaw support but are less aesthetic.
Q: I finished braces and my jaw popping came back. Why?
A: The three most common reasons are: 1) Not wearing retainers, allowing teeth/bite to shift. 2) Unresolved nighttime grinding/clenching putting pressure on the joint. 3) Eruption of wisdom teeth destabilizing the dental arch.
Q: Can elastics (rubber bands) make my jaw popping worse?
A: Yes, temporarily. Class II elastics (pulling lower jaw forward) or Class III elastics (pulling upper jaw forward) change the position of the condyle. This can cause a temporary “searching” pop. Never stop wearing elastics due to popping without consulting your orthodontist, as the pop is often part of the therapeutic repositioning process.
Q: Is jaw surgery the only option if braces don’t stop the popping?
A: No. If braces fail to stop the popping, it usually indicates the problem is inside the joint capsule, not the teeth. Options include arthrocentesis (washing out the joint), steroid injections, or arthroscopy. Jaw surgery is reserved for severe skeletal deformities or advanced degenerative disease.
Additional Resources
For further reading on the relationship between orthodontics and temporomandibular disorders, please visit the official resource page of the American Association of Orthodontists (AAO) .