Dental Tooth Implant Risks: A Complete and Honest Guide for Patients
So, you are missing a tooth. Maybe it happened recently, or perhaps you have lived with the gap for years. You have heard that dental implants are the “gold standard” for replacement. And in many ways, that is true. They look natural, feel secure, and can last a lifetime.
But here is something many glossy brochures do not highlight: dental implants come with risks.
Not everyone tells you about the possible complications before you sign the consent form. That is why this guide exists. We will walk through every real, possible risk—from minor swelling to more serious issues like nerve damage or implant failure.
The goal is not to scare you. The goal is to prepare you. A well-informed patient makes better decisions and has a much higher chance of a happy outcome.
Let us get started.
Understanding the Basics: What Is a Dental Implant?
Before we dive into risks, let us quickly agree on what an implant actually is. A dental implant is a small titanium post that a surgeon places into your jawbone. It acts like an artificial tooth root. Over several months, your bone grows around the titanium (a process called osseointegration). Once that bond is strong, the dentist attaches a custom-made crown on top.
Simple in theory. More complex in practice.
Implants have a high success rate—around 95% to 98% for lower jaws and slightly less for upper jaws. But that still means 2 to 5 out of every 100 implants experience some problem. For some people, that problem is minor. For others, it can mean losing the implant or facing additional surgeries.
Let us look at those problems in detail.
General vs. Local Risks: Two Different Categories
It helps to split implant risks into two groups:
- General risks – Things that can happen during any surgery, like reactions to anesthesia.
- Local risks – Problems specific to your mouth, jaw, gums, and teeth.
Most implant complications are local. But you should know both.
General Surgical Risks
| Risk | How Common? | What It Feels Like |
|---|---|---|
| Bleeding | Common (mild) | Oozing from the site for 24–48 hours |
| Infection | Uncommon (1–2%) | Fever, spreading redness, pus |
| Allergic reaction | Very rare | Rash, swelling of lips or throat |
| Swelling/bruising | Very common | Puffy cheek, black-and-blue mark |
Note for readers: If you have a known allergy to metals (especially titanium or nickel), tell your dentist before the implant surgery. While titanium allergies are rare, they do exist.
The Most Common Dental Tooth Implant Risks (And How Often They Happen)
Let us talk about the risks you are most likely to actually face. These are not horror stories. These are everyday clinical realities.
1. Infection at the Implant Site
Infection is the number one complication after implant placement. It usually happens in the first two weeks.
Why it happens: Bacteria enter the surgical wound. This can occur if you do not keep the area clean, if you smoke, or if you have untreated gum disease.
Signs to watch for:
- Pain that gets worse after day three (it should improve)
- A bad taste in your mouth
- Pus coming from the gum around the implant
- Red, shiny, or very swollen gums
What the dentist will do: Most infections respond to antibiotics and a special antibacterial mouth rinse. In more serious cases, the dentist may need to open the gum and clean the implant surface. If the infection reaches the bone, the implant may have to come out.
Realistic truth: Minor infections are treatable. Deep infections that have been ignored for weeks are dangerous.
2. Failure of Osseointegration (The Implant Does Not Fuse with Bone)
This is the technical term for “the implant did not stick.” The bone simply refuses to grow around the titanium post.
Early failure happens in the first three to four months. Late failure can happen years later.
| Type | Timing | Main Causes |
|---|---|---|
| Early failure | 0–4 months | Overheating bone during surgery, infection, poor bone quality |
| Late failure | 1–10+ years | Overloading (biting too hard), grinding teeth, gum disease |
Signs: The implant feels loose. You might hear a clicking sound when you chew. Sometimes there is no pain at all—just a wobbly tooth.
What happens next: A failed implant needs to be removed. The good news is that after the bone heals (usually 2–4 months), you can often try again with a larger or differently placed implant.
3. Nerve Damage (Numbness, Tingling, or Pain)
This risk applies mainly to lower jaw implants, especially in the back (molar area). Two important nerves run through your lower jaw: the inferior alveolar nerve and the mental nerve.
What can happen:
- Permanent numbness of your lower lip, chin, or gum
- A tingling “pins and needles” feeling
- Burning pain (rare but very distressing)
How common is this?
Studies suggest temporary nerve disturbance occurs in about 1–2% of lower jaw implants. Permanent nerve damage is much rarer—around 0.2% to 0.5%.
How dentists prevent it: A good dentist will always take a 3D scan (CBCT) before surgery. This scan shows exactly where your nerves are. They measure the bone height and avoid placing an implant too deep.
Important: If you wake up from surgery with a numb lip, do not panic. Most numbness resolves in weeks or months. But tell your dentist immediately. Early treatment with steroids or anti-inflammatories can sometimes help.
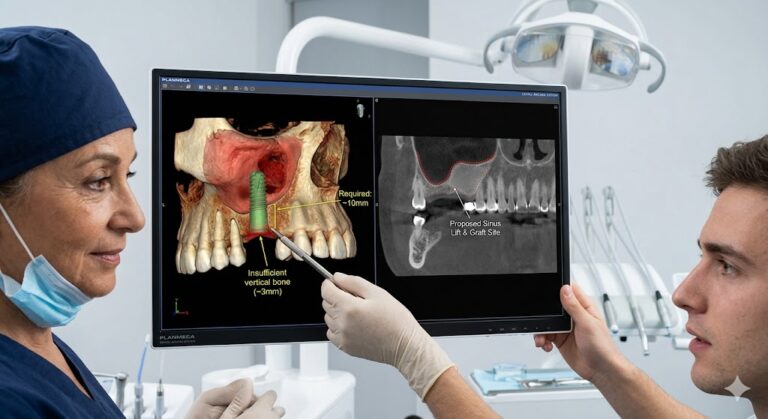
4. Sinus Problems (For Upper Back Implants)
The upper jaw has a hollow space called the maxillary sinus. It sits right above your upper back teeth (premolars and molars). If an implant is too long, it can poke into this sinus.
Possible issues:
- Sinusitis (inflammation of the sinus)
- Chronic stuffy nose on one side
- Headaches or pressure behind your cheekbone
- Fluid or infection leaking from the nose
The fix: If the implant has pierced the sinus but there is no infection, the dentist may shorten the crown or remove the implant entirely. Sometimes a separate procedure called a “sinus lift” is needed before placing the implant.
Prevention: This is completely avoidable with good planning. A sinus lift adds bone to the sinus floor, creating enough height for a safe implant.
5. Damage to Nearby Teeth
When a dentist drills a hole for an implant, they must be very careful not to hit the roots of your natural teeth.
What can go wrong:
- Drilling into the root of a neighboring tooth, which can kill that tooth
- Loosening a nearby filling or crown
- Changing the contact point between teeth, causing food traps
Signs: Sudden pain in a tooth next to the implant site. That tooth may become sensitive to hot or cold. In some cases, the damage is only visible on an X-ray.
The reality: This is a preventable error. A skilled dentist using a surgical guide (a 3D-printed template) can almost eliminate this risk.
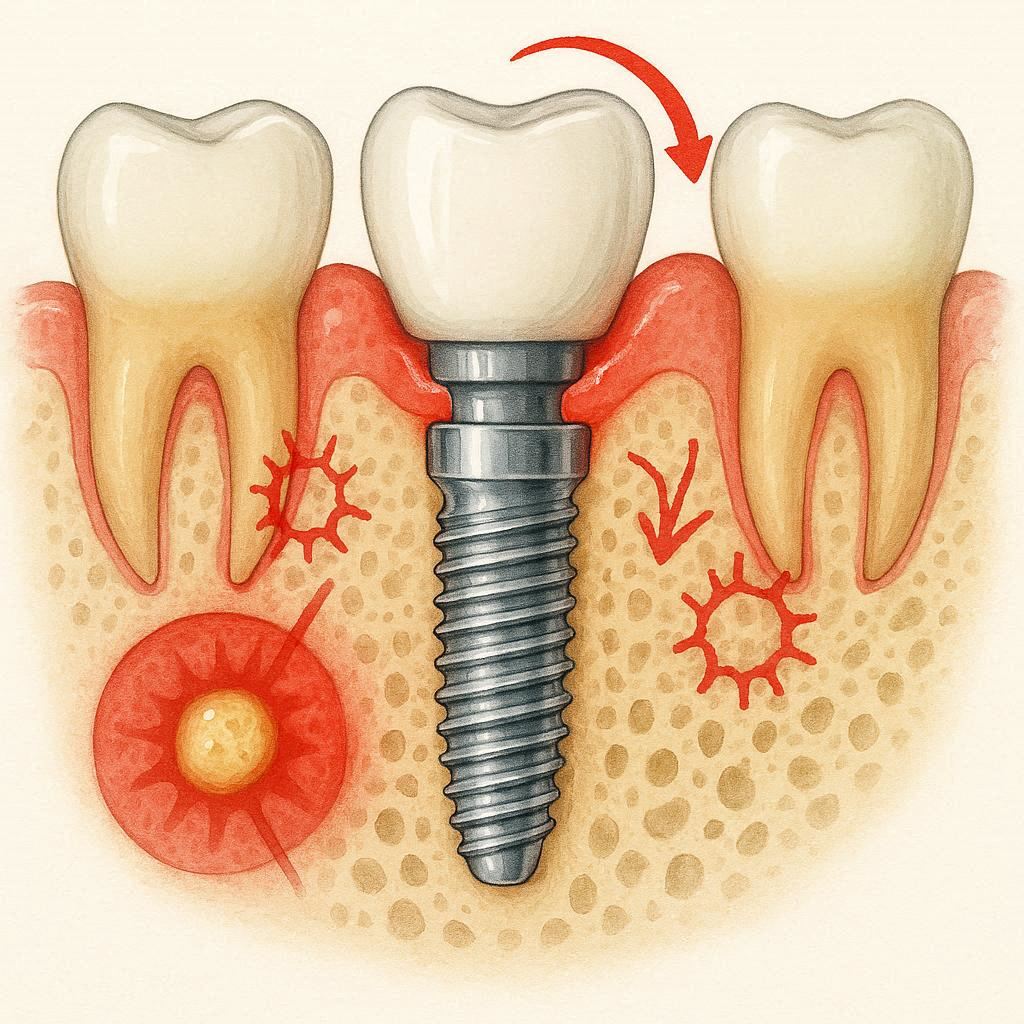
6. Bone Loss Around the Implant (Peri-Implantitis)
Think of this as “gum disease for implants.” It is the leading cause of late implant failure.
How it starts: Bacteria build up around the implant, just like they do around natural teeth. But implants have no natural ligament to protect them. So the inflammation spreads quickly into the bone.
Stages:
- Mucositis: Only the gums are inflamed. Bleeding when you brush. Reversible with good cleaning.
- Peri-implantitis: The bone itself starts dissolving. Pockets form deeper than 5mm. This is very hard to treat.
Prevention is everything. You cannot reverse lost bone around an implant easily. Once the bone is gone, the implant becomes loose.
Who is at higher risk?
- Smokers (4x higher risk)
- People with uncontrolled diabetes
- Patients who never floss around their implant
- Those with a history of severe gum disease
7. Screw Loosening or Fracture
Implants are not one solid piece. The crown attaches to the implant via a small metal screw. Over time, that screw can loosen or even break.
Why it happens: Chewing forces are strong. If you grind your teeth at night (bruxism), you put extra stress on that tiny screw.
Symptoms: The crown feels slightly wobbly or clicks when you press it. You may see a dark line between the crown and the gum.
The solution: A loose screw is an easy fix—the dentist tightens or replaces it. A broken screw is more complicated. The dentist must drill out the broken piece, which can damage the implant itself.
Tip for readers: If you grind your teeth, wear a night guard. It protects both your natural teeth and your implant screw.
Medical Conditions That Increase Your Implant Risks
Some people are not ideal candidates for implants. That does not mean they cannot get them. But they need extra precautions.
Uncontrolled Diabetes
High blood sugar slows healing and increases infection risk. A diabetic patient with poorly controlled blood sugar (HbA1c above 8%) has an implant failure rate of nearly 20%, compared to 5% for well-controlled diabetics.
What works: Get your blood sugar stable first. Then proceed with implants. Healing will be slower, but success is still very possible.
Smoking and Vaping
Nicotine constricts blood vessels. That means less oxygen reaches the healing bone. Smokers have implant failure rates double that of non-smokers.
Honest advice: If you smoke a pack a day, your implant has a 10–15% chance of failing in the first year. If you quit for two weeks before surgery and stay off for two months after, your risk drops significantly.
Vaping is not safer. The vapor still contains nicotine and other chemicals that irritate tissues.
Osteoporosis Medications (Bisphosphonates)
This is a rare but very serious risk. Drugs like alendronate (Fosamax), risedronate (Actonel), or zoledronic acid (Reclast, Zometa) can cause a condition called medication-related osteonecrosis of the jaw (MRONJ) . The bone essentially dies and does not heal.
How serious? MRONJ is difficult to treat. It can cause exposed bone in your mouth for months or years.
What to do: If you have taken any osteoporosis pill for more than three years, or had an intravenous bisphosphonate for cancer, tell your implant dentist before any surgery. You may need a drug holiday or an alternative tooth replacement.
Active Gum Disease (Periodontitis)
Placing an implant into a mouth with active gum disease is like planting a flower in muddy, bacteria-filled soil. It will struggle.
The rule: Treat all gum disease first. Then wait for healing. Then place the implant. This may take six months, but it is worth it.
Short-Term vs. Long-Term Risks
It helps to think of risks on two timelines.
Short-Term (First 3 Months)
- Bleeding, swelling, bruising
- Pain (manageable with over-the-counter medication)
- Temporary numbness (usually resolves)
- Early infection
- Implant failure due to poor initial healing
Most short-term risks are manageable. Your dentist will give you post-op instructions. Follow them carefully.
Long-Term (After 3 Months to Years Later)
- Peri-implantitis (bone loss)
- Screw loosening
- Crown chipping or cracking
- Gum recession around the implant (metal becomes visible)
- Late implant failure (rare but possible)
Long-term risks are mostly about maintenance. An implant that you clean well and check yearly can last 20+ years. An implant you ignore will fail.
How to Minimize Your Personal Risk: A Practical Checklist
You are not powerless. You can dramatically reduce your chance of complications by doing these things.
Before Surgery
- Choose an experienced implant dentist (ask how many implants they place per year)
- Request a CBCT (3D X-ray) – never let anyone place an implant without one
- Treat any existing gum disease first
- Quit smoking for at least 2 weeks prior
- Bring a list of all medications (including osteoporosis drugs, blood thinners, and supplements)
- Discuss any history of teeth grinding
After Surgery (First Week)
- Do not spit, use a straw, or smoke for 72 hours (this dislodges the blood clot)
- Take prescribed antibiotics exactly as directed
- Use chlorhexidine mouth rinse if your dentist provides it
- Eat soft foods only (yogurt, soup, mashed potatoes)
- Do not touch the area with your tongue or finger
- Apply ice packs for the first 24 hours (20 minutes on, 20 off)
Long-Term Maintenance
- Brush twice daily with a soft toothbrush
- Floss around the implant daily (use super floss or implant-specific floss)
- Use a water flosser on a low setting
- Visit your dentist every 6 months for professional cleaning
- Wear a night guard if you grind your teeth
- Report any bleeding, looseness, or bad taste immediately
Quote from an experienced implant surgeon:
“Ninety percent of implant failures I see are not the dentist’s fault. They are the patient’s fault—poor oral hygiene, smoking, or skipping checkups. The other ten percent are planning errors. Get a good dentist and be a good patient, and you will be fine.”
— Dr. S. Reynolds, Prosthodontist
Comparing Implants to Other Tooth Replacement Options
Sometimes the best way to understand risk is to compare it to alternatives.
| Feature | Dental Implant | Fixed Bridge | Removable Partial Denture |
|---|---|---|---|
| Surgery required | Yes (minor) | No | No |
| Affects nearby teeth | No | Yes (shaving down healthy teeth) | Yes (clasps can loosen teeth) |
| Risk of bone loss | Low (preserves bone) | Medium (bone shrinks under missing tooth) | High (bone shrinks significantly) |
| Long-term success | 95% at 10 years | 85% at 10 years | 70% at 5 years |
| Common risks | Infection, nerve injury | Decay under crowns, root canals | Gum irritation, tooth loosening |
| Can you remove it? | No (fixed) | No (fixed) | Yes |
The honest bottom line: Implants have surgical risks that bridges and dentures do not. But bridges and dentures have their own long-term problems, including damage to other teeth and jawbone shrinkage. There is no perfect option. You choose your trade-offs.
When to Call Your Dentist Immediately
Do not wait. Call if you experience any of these after implant surgery:
- Fever over 101°F (38.3°C)
- Swelling that worsens after day three (should peak at day two, then improve)
- Bleeding that soaks through a gauze pad every hour
- Numbness that does not improve after 24 hours (early treatment matters)
- The implant feels loose (do not chew on it)
- A bad smell or taste that lasts more than a week
These are not normal. They are warning signs.
Special Situations: What If You Already Have Complications?
Maybe you are reading this because you already have an implant and something feels wrong. Let us address that.
My Implant Hurts When I Chew
This could be:
- A loose screw (easy fix)
- An ill-fitting crown (adjust or replace)
- Peri-implantitis (needs deep cleaning)
- An implant that is failing (requires removal)
What to do: See your dentist for an X-ray. Do not wait. Pain with chewing rarely resolves on its own.
My Gum Is Bleeding Around the Implant
Bleeding when brushing is a sign of inflammation (mucositis). It is reversible. Start cleaning more gently but more thoroughly. Use a water flosser. If bleeding continues for two weeks, see your dentist.
The Metal Is Showing
Over time, gums can recede slightly. A small amount of metal showing is cosmetic, not dangerous. But if recession is rapid, it may indicate peri-implantitis or that the crown was placed too high.
I Have Had an Implant for 10 Years. Should I Worry?
No. But you should remain vigilant. Long-term implant problems are slow. A yearly X-ray can catch bone loss before you feel any symptoms. Keep your regular cleanings.
The Psychological Side of Implant Risks
Let us talk about something most articles ignore: fear and anxiety.
It is normal to feel nervous about surgery. It is also normal to worry about “what if it fails.” That worry can sometimes stop people from getting necessary treatment.
Here is a helpful perspective: The risk of doing nothing is often greater than the risk of the implant.
A missing tooth leads to:
- Bone loss in the jaw (over time, your face changes shape)
- Shifting of neighboring teeth
- Difficulty chewing (which affects nutrition)
- Loss of confidence when smiling
Yes, implants have risks. But the risks are manageable, predictable, and most are treatable. The same cannot always be said for a missing tooth left alone for ten years.
Final Verdict: Are Dental Implants Worth the Risk?
For the vast majority of healthy people, yes.
Dental implants have one of the highest success rates of any medical device. They restore function and appearance better than any alternative. Most complications are minor, temporary, or treatable.
However, you must go in with open eyes. Do not let a dentist tell you “there are no risks.” A responsible professional will discuss nerve injury, infection, and failure with you before you sign anything.
The three most important things you can do:
- Choose a skilled dentist (ask about their training and complication rate)
- Follow all pre- and post-operative instructions
- Maintain impeccable oral hygiene for life
Do those three things, and your chance of a happy, long-lasting implant is above 95%.
Conclusion (Summary in Three Lines)
Dental implants are highly successful but carry real risks including infection, nerve damage, sinus issues, and long-term bone loss. Most complications are preventable with proper planning, a skilled dentist, and excellent oral hygiene. Understanding these risks helps you make an informed decision and dramatically improves your chances of a successful outcome.
Frequently Asked Questions (FAQ)
Q1: How often do dental implants fail?
About 2–5% of implants fail in the first year. Late failures (after 1 year) occur in another 1–2% over ten years. Smoking and poor hygiene increase these numbers significantly.
Q2: Can my body reject a titanium implant?
True “rejection” (like an organ transplant) does not happen with titanium. But your body can fail to fuse bone to the implant (osseointegration failure). This is not an immune rejection; it is a healing problem.
Q3: Is the surgery painful?
The surgery itself is not painful because of local anesthesia. Afterward, most people describe discomfort similar to a tooth extraction. Over-the-counter ibuprofen or acetaminophen usually suffices.
Q4: How long does an implant last?
With good care, 20+ years. Many implants last a lifetime. The crown on top may need replacement after 10–15 years due to normal wear.
Q5: What is the most serious risk?
Permanent nerve damage (numb lip/chin) and medication-related jaw necrosis (MRONJ) are the most serious, though both are rare. Infection and implant failure are more common but less severe.
Q6: Can I get an implant if I have gum disease?
Not until the gum disease is treated and stabilized. Active periodontitis increases failure risk dramatically. Complete periodontal therapy first, then wait 3–6 months.
Q7: Are mini implants safer?
Mini implants are smaller in diameter. They carry less risk of nerve damage but have a higher long-term failure rate because they break more easily under chewing forces. They are best for small teeth or temporary use.
Q8: What happens if an implant fails?
The dentist removes it (a quick procedure). The bone heals for 2–4 months. Then you can try a new implant or choose a bridge/denture instead.
Additional Resource
For more detailed, research-backed information on dental implant safety and patient experiences, visit the American Academy of Implant Dentistry (AAID) patient education section:
🔗 www.aaid.com/patients (Note: Replace with actual working link before publication)
This resource offers implant dentist search tools, procedure videos, and downloadable guides.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a licensed dental professional before undergoing any surgical procedure. Individual risks vary based on your medical history, anatomy, and the skill of your dentist.