The True Cost of Dental Implant Failure: A Comprehensive Guide to Financial, Health, and Emotional Repercussions
Imagine investing thousands of dollars, hours of your time, and your trust in a medical procedure promised to restore your smile, your confidence, and your ability to eat comfortably for a lifetime. You endure the surgery, the healing process, and finally, you receive the crown—a perfect, permanent tooth. For months or even years, it functions flawlessly. Then, a subtle ache emerges. A faint wiggle. A strange taste. The dreaded diagnosis follows: implant failure. Your investment, both financial and emotional, now sits on the precipice of collapse. This scenario is not a rare nightmare; it is a complex and costly reality for a significant number of patients. The conversation around dental implants almost universally focuses on success rates—often cited at 95% or higher. While statistically accurate, this figure obscures a critical narrative: for the 5% or more who experience failure, the consequences are profound, multidimensional, and devastatingly expensive. The true cost of dental implant failure extends far beyond the initial price tag. It is a labyrinth of secondary surgical procedures, additional restorative work, bone grafting complexities, specialist referrals, lost wages, psychological distress, and the daunting prospect of starting from square one. This article, exclusive in its depth and scope, will dissect every layer of this crisis. We will move beyond simplistic explanations to explore the biomechanical, biological, and behavioral causes of failure, quantify the staggering financial repercussions, and provide an actionable roadmap for prevention and remediation. If you are considering an implant or are currently navigating the distress of a failing one, this is your essential guide to understanding, mitigating, and surviving one of dentistry’s most significant challenges.

1. Understanding Dental Implant Failure: Definitions and Classifications
Not all failures are created equal, and the timing of the failure dictates its cause, treatment, and cost. The dental community broadly classifies implant failure into two distinct categories: early (or biological) failure and late (or mechanical) failure.
Early Failure occurs before the implant has had a chance to osseointegrate—the critical process where the titanium fixture fuses directly with the jawbone. This typically happens within the first few months to a year of placement. Causes are often biological or surgical: poor blood supply, infection at the time of surgery (contamination), premature loading (putting pressure on it too soon), or systemic patient factors like uncontrolled diabetes or heavy smoking that impede healing. The implant is essentially rejected by the body or fails to bond. The sensation is often a loose implant, sometimes with discomfort or signs of infection.
Late Failure happens after successful osseointegration, often years later. The primary villain here is typically peri-implantitis—a destructive inflammatory process affecting the soft and hard tissues surrounding the implant, analogous to periodontitis around a natural tooth. It is characterized by bleeding, pus, progressive bone loss, and the formation of a pathological pocket. If unchecked, it leads to the loss of integration and ultimate failure. Other causes include chronic overload from bruxism (teeth grinding), a fractured implant screw or abutment, or a fracture of the implant fixture itself.
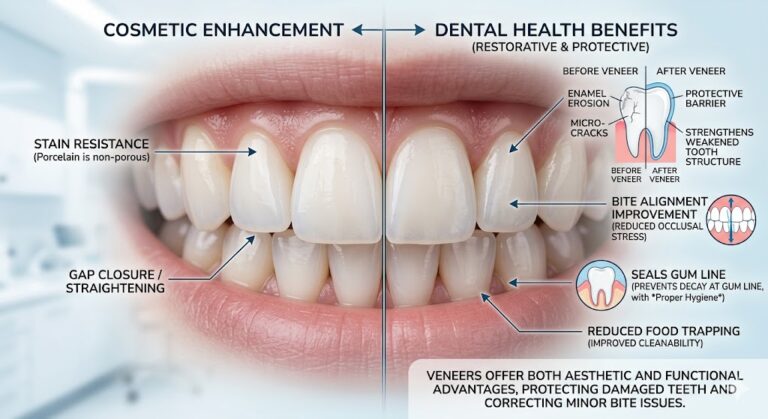
A third, often-overlooked category is esthetic failure. Here, the implant is functionally integrated and healthy but results in an unsatisfactory appearance due to gum recession, poor prosthetic shape, or color mismatch. While not a “failure” in the structural sense, it often necessitates costly corrective procedures to achieve the promised result, representing a significant financial and emotional cost.
2. The Biological Price Tag: Peri-Implantitis and Bone Loss
Peri-implantitis is the single greatest threat to the long-term survival of dental implants and the most common cause of late failure. It is a biofilm-driven infection, but its progression can be more aggressive and harder to treat than periodontal disease. The cost trajectory of peri-implantitis is a steep curve.
Stage 1: Diagnosis and Non-Surgical Therapy. The first sign may be bleeding on probing. A diagnosis requires radiographic evidence of bone loss beyond initial remodeling. Initial treatment mirrors periodontal therapy: specialized debridement of the implant surface using titanium or plastic scalers, antiseptic irrigation, and possibly localized antibiotics. Cost: $500 – $1,500 per implant.
Stage 2: Surgical Intervention. If non-surgical methods fail, surgical access is required. This involves reflecting a gum flap to directly visualize and clean the contaminated implant surface. Advanced techniques like regenerative surgery may be attempted using bone grafts and membranes to try to rebuild lost bone. Success is not guaranteed. Cost: $2,000 – $5,000+ per implant.
Stage 3: Explanation and Site Reconstruction. When the infection has caused severe bone destruction, the implant must be removed. The explantation procedure itself can be simple or complex, requiring trephine burs to cut out the implant. The resulting bone defect is often substantial, requiring significant bone grafting (often block grafts or sophisticated techniques like guided bone regeneration) to rebuild the site for a future implant. This stage essentially resets the clock to a pre-implant condition, but with compromised anatomy. Cost: $1,500 – $3,000 for removal, plus $2,000 – $6,000+ for bone grafting.
The Cumulative Biological Cost: A single implant battling peri-implantitis can easily incur $10,000 – $15,000+ in remedial treatments over several years before a new implant can even be considered.
*[Image: A comparative radiograph series showing progressive bone loss around an implant over a 5-year period.]*
3. The Mechanical Bill: Fractures, Overload, and Component Failure
When the biological environment is stable, mechanical forces can become the point of failure. The implant system is a complex assembly: the fixture (in the bone), the abutment (the connector), and the prosthetic crown (the visible tooth). Any link can break.
Abutment or Prosthetic Screw Fracture: The most common mechanical issue. It is often retrievable by drilling out the broken screw and replacing it, but requires skill and specialized kits. Cost: $500 – $1,500.
Abutment Fracture: Less common, but requires removal of the crown and possibly the fractured abutment segment. A new custom abutment and crown are typically needed. Cost: $1,500 – $3,500.
Implant Fixture Fracture: The catastrophic failure. It is rare but almost always requires removal of the fractured implant, which can be surgically challenging. The cause is usually chronic excessive force (bruxism) or a manufacturing defect. The cost involves complex explanation and major site reconstruction. Cost: $2,500 – $7,000+ for removal and grafting.
The Role of Bruxism: Untreated nighttime clenching and grinding places immense, off-axis forces on implants. This can cause screw loosening, porcelain fracture on the crown, and eventually bone loss or fixture fracture. The cost of failure here must include the cost of the preventative measure: a custom-fitted night guard ($500 – $1,500), which is a negligible investment compared to the repairs it prevents.
4. The Surgical Ledger: Technical Errors and Anatomical Challenges
The foundation of implant success is laid during surgery. Errors here, while sometimes unavoidable due to anatomy, can doom an implant from the start.
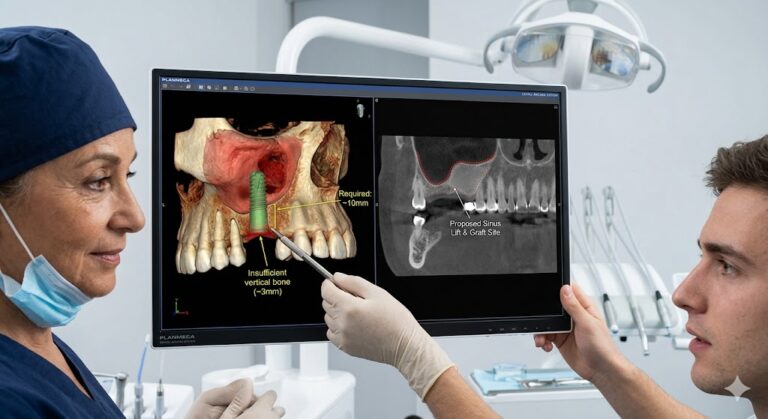
Poor Implant Positioning: Placement too close to a nerve can cause permanent paresthesia (numbness). Placement with poor angulation makes for an unrestorable implant or one that is chronically uncleanable, inviting peri-implantitis. Corrective surgery often requires removal. Cost of corrective sinus lift or nerve repair: $2,000 – $5,000. Cost of malpractice litigation: potentially limitless.
Insufficient Bone Volume: Placing an implant in inadequate bone without proper grafting leads to poor primary stability and early failure. The surgeon must assess bone quality (Density classified as D1-D4) and quantity via 3D CBCT scan pre-operatively. Skipping this step is a major risk factor. Cost of a CBCT scan: $250 – $500—an essential diagnostic investment.
Surgical Trauma & Thermal Injury: Overheating the bone during drilling without proper irrigation causes necrosis (death) of bone cells, preventing osseointegration. This is a technique-sensitive error.
Comparative Cost Analysis of Implant Success vs. Failure Scenarios
| Scenario | Initial Procedure Cost (Avg.) | Remediation/Additional Procedures | Estimated Total Cost | Time Investment |
|---|---|---|---|---|
| Uncomplicated Success | $3,000 – $6,000 (single implant) | None (only routine maintenance) | $3,000 – $6,000 | 4-12 months |
| Early Failure & Replacement | $4,000 | Removal ($1,500), Bone Graft ($2,500), New Implant/Crown ($4,000) | $8,000+ | 18-24+ months |
| Late Failure (Peri-implantitis) | $5,000 | Non-Surgical Therapy ($1,000), Surgical Therapy ($3,500), Failure leads to Removal ($2k) & Graft ($4k) | $15,500+ | 2-3+ years of treatment |
| Mechanical Failure (Fractured Fixture) | $4,500 | Complex Removal ($3,000), Major Bone Graft ($5,000), New Implant/Crown ($4,500) | $17,000+ | 24-36 months |
| Esthetic Failure | $5,500 | Pink Porcelain/Gum Grafting ($2,000), New Custom Abutment & Crown ($3,000) | $10,500 | 6-12 months |
5. The Patient’s Contribution: Lifestyle and Systemic Health Factors
The patient is not a passive recipient. Long-term success is a partnership, and patient choices directly impact the risk of failure.
Smoking: Nicotine vasoconstricts blood vessels, severely reducing blood flow and oxygen delivery to the surgical site. This impairs healing, increases infection risk, and is one of the most significant risk factors for peri-implantitis. Studies show failure rates can double or triple for smokers.
Uncontrolled Diabetes: Hyperglycemia impairs neutrophil function (white blood cells) and collagen synthesis, slowing healing and increasing susceptibility to infection. Tight glycemic control is essential before and after surgery.
Poor Oral Hygiene: Implants, unlike teeth, have no periodontal ligament. The gum attachment is weaker, making the seal more vulnerable. Plaque accumulation leads swiftly to mucositis (gum inflammation), the precursor to peri-implantitis. The cost of negligence is the cost of failure.
Lack of Compliance with Maintenance: The “placement and forget” mindset is a path to disaster. Professional implant maintenance visits every 3-6 months, using appropriate instruments, are non-negotiable. Annual maintenance cost: $200 – $600. Compare this to the cost of treating peri-implantitis.
6. The Direct Financial Costs: A Line-Item Catastrophe
Let’s synthesize the previous sections into a stark, itemized invoice for a hypothetical late failure case (Peri-implantitis leading to explanation):
-
Initial Implant & Crown (5 years prior): $4,800
-
Diagnostic Records for Problem (CBCT, photos): $450
-
Non-Surgical Peri-Implantitis Therapy: $850
-
Surgical Peri-Implantitis Therapy (resective): $3,200
-
Implant Removal Surgery (due to progression): $1,800
-
Bone Grafting Procedure (block graft): $4,500
-
Healing Period (6+ months) with Temporary Tooth: $600
-
New Implant Placement (second attempt): $3,500
-
New Abutment and Crown: $2,300
-
SUBTOTAL (Procedural): $22,000
-
Lost Wages (5-7 days off work across procedures): $1,500 – $3,000
-
Prescription Medications, Special Supplies: $300
-
Travel/Parking for numerous appointments: $400
-
ESTIMATED GRAND TOTAL: $24,200 – $25,700
This figure, nearly five times the original cost, illustrates the profound financial gravity of failure. And this assumes the second attempt is successful.
7. The Indirect and Intangible Costs: Time, Pain, and Lost Opportunity
The financial numbers, though staggering, tell only half the story.
-
Time: An implant journey stretches from 4-12 months. A failure journey can span 2-4 years of repeated surgeries, healing periods, and countless appointments.
-
Physical Discomfort and Pain: Each surgical intervention brings renewed cycles of swelling, pain, dietary restrictions (soft foods), and the mental fatigue of convalescence.
-
Psychological Impact: The emotional toll is severe. Patients report feelings of betrayal, anxiety, depression, and a loss of confidence. The promised “permanent solution” has failed, creating a crisis of trust in dental professionals and fear of future procedures.
-
Social and Professional Detriments: Gaps in one’s smile during lengthy repair processes can affect self-esteem in social interactions and professional settings, potentially impacting careers.
8. The Insurance Quaghem: What is (and isn’t Covered)
Dental insurance is a minefield in the best of times; with implant failure, it becomes almost adversarial. Key points:
-
Initial Implant: Often has limited coverage (50% or less of a “usual and customary” fee, which is below market rate) with annual maximums ($1,000-$1,500) that barely dent the cost.
-
Treatment of Failure: Procedures deemed “corrective” or due to “complications” may be outright denied. Insurance language often excludes coverage for re-treatment.
-
Bone Grafting & Site Prep: May be covered under the initial surgical benefit, but again, subject to limitations and deductibles.
-
Medical Insurance: May rarely contribute if failure is linked to a traumatic accident or a specific covered medical condition, but almost never for standard biological/mechanical failure.
-
Warranties: Some high-quality dental practices or implant manufacturers offer limited long-term warranties (e.g., 5-10 years) on the implant fixture itself, but these typically cover replacement of the component only, not the labor for removal, grafting, and new crown. Read the warranty fine print meticulously.
9. Prevention: The Ultimate Cost-Saving Strategy
An ounce of prevention is worth tens of thousands of dollars in cure. The protocol for preventing failure is a continuous thread from pre-planning to lifelong care.
Phase 1: The Pre-Implant Investment (The Foundation)
-
Comprehensive Diagnosis: Insist on a CBCT 3D scan and thorough periodontal evaluation.
-
Select the Right Team: Choose an experienced, credentialed surgeon (e.g., a periodontist or oral surgeon) and a skilled restorative dentist. Don’t shop on price alone.
-
Optimize Your Health: Quit smoking. Get diabetes under control. Address gum disease before implant placement.
-
Plan for the Final Tooth: The restorative dentist should drive the plan via a “restoratively driven” approach, often using surgical guides.
Phase 2: The Surgical & Healing Phase (The Installation)
-
Meticulous Surgical Protocol: Sterile technique, appropriate implant selection, precise placement.
-
Adequate Healing Time: Respect the osseointegration period before loading, especially in soft bone.
Phase 3: The Lifelong Maintenance Phase (The Preservation)
-
Impeccable Home Care: Use soft brushes, nylon-coated interdental brushes, and water flossers designed for implants.
-
Professional Maintenance: Schedule peri-implant maintenance every 3-6 months. This is different from a regular cleaning and involves monitoring pocket depths, assessing occlusion, and using instruments that won’t scratch the titanium.
-
Wear Your Night Guard: If you have bruxism, this is mandatory insurance.
10. Salvage vs. Removal: The Crossroads of Remediation
When failure is diagnosed, the first critical decision is: can we save it?
Salvage (Rescue Therapy) is attempted when there is moderate bone loss but the implant is still stable. The goal is to arrest disease progression via the therapies described in Section 2. Success is defined as arrested progression, not necessarily bone regeneration. The decision to attempt salvage weighs the cost of repeated therapies against the cost and ordeal of removal and replacement.
Removal (Explantation) is indicated when:
-
Implant mobility is present (loss of integration).
-
Bone loss is severe (>50% of the implant length).
-
The implant is in a hopeless position (causing nerve damage, chronic infection, or is unrestorable).
-
Salvage therapies have failed.
The decision is complex and must involve a specialist, typically a periodontist, using 3D imaging and clinical findings.
11. Legal and Ethical Considerations: Who Bears the Cost?
When failure occurs, the question of responsibility arises. Was it an unavoidable biological response, a consequence of patient non-compliance, or the result of professional negligence?
-
Standard of Care: Did the provider meet the accepted standard in diagnosis, planning, execution, and informed consent? Failure to use a CBCT for complex cases, for example, could be seen as a deviation.
-
Informed Consent: Were the risks of failure, including smoking, diabetes, and bruxism, clearly documented and discussed with the patient? A robust consent process is a medico-legal necessity.
-
Warranties and Guarantees: Be wary of clinics offering “lifetime guarantees.” Understand what is covered (parts only vs. labor) and the conditions (mandatory maintenance visits, etc.).
-
Mediation and Litigation: Pursuing legal action is costly, time-consuming, and emotionally draining. It is generally only advisable in clear cases of gross negligence or breach of contract. The first step is always a direct, documented conversation with the provider.
12. Conclusion: Protecting Your Investment and Your Health
The journey of a dental implant is a profound investment in oneself. Its potential failure represents not just a financial catastrophe, but a physical and emotional ordeal. The true cost, as we have seen, is measured in repeated surgeries, lost time, and shattered confidence. You can dramatically mitigate this risk by being an empowered, proactive participant: choose your clinical team with rigorous care, invest in comprehensive diagnostics, uncompromisingly optimize your systemic and oral health, and commit to a lifelong pact of meticulous professional maintenance. View the implant not as an indestructible device, but as a biomechanical masterpiece that requires vigilant stewardship. In doing so, you protect not only your financial outlay but your health, your smile, and your peace of mind for decades to come.
13. Frequently Asked Questions (FAQs)
Q1: What are the very first signs of a failing dental implant?
A: Early signs include redness, swelling, or tenderness in the gums around the implant, bleeding when brushing or probing, a persistent bad taste or smell, and gradual gum recession. A loose feeling crown or implant is a more advanced sign requiring immediate attention.
Q2: My implant failed. Will my dentist/surgeon fix it for free?
A: This depends on the cause, the warranty provided, and the practice’s policies. If failure is due to a surgical error or component defect, a reputable provider may cover some or all costs of remediation. If it’s due to patient-related factors (smoking, poor hygiene, untreated bruxism), they are unlikely to bear the cost. Review your initial contract and warranty documents.
Q3: How long after an implant fails can I get a new one?
A: It’s almost never immediate. The failed implant must be removed, and the site must heal, often requiring bone grafting. The graft then needs 4-9 months to mature before a new implant can be placed. The entire process from failure to a new restored implant typically takes a minimum of 12-18 months.
Q4: Is dental implant failure a sign of malpractice?
A: Not necessarily. Implants have a known statistical failure rate, and many failures are due to complex biological responses or patient factors. Malpractice would involve a clear deviation from the standard of care (e.g., placing an implant into a major nerve without a CT scan, using improper sterile technique).
Q5: Can a failed implant be saved?
A: Sometimes, especially in cases of early peri-implantitis. With aggressive professional treatment and impeccable home care, the disease process can be arrested. However, once significant bone loss or mobility occurs, salvage becomes less likely, and removal is often the only viable option.
Q6: Are “cheap” dental implants more likely to fail?
A: Cost is a proxy for many things: the experience of the team, the quality of diagnostics (CBCT vs. simple X-ray), the time taken, the brand of implant components (with proven research), and the quality of the dental lab crafting the crown. Cutting corners in any of these areas increases risk. The old adage, “you get what you pay for,” holds significant truth in implant dentistry.
14. Additional Resources
-
Academy of Osseointegration (AO): A premier multidisciplinary organization for implant dentistry. Their public website offers patient-focused information and finding a clinician. https://www.osseo.org/
-
American Academy of Periodontology (AAP): The leading authority on gum health and disease, including peri-implant diseases. Their site includes explanations of diseases and a “Find a Periodontist” tool. https://www.perio.org/
-
International Congress of Oral Implantologists (ICOI): A global organization offering patient education and a clinician finder. https://www.icoi.org/
-
National Institute of Dental and Craniofacial Research (NIDCR): Provides science-based information on dental implants and oral health. https://www.nidcr.nih.gov/health-info/dental-implants
-
PubMed.gov: A database of medical literature. Searching for “peri-implantitis treatment” or “dental implant failure risk factors” can provide access to current research (articles are often technical).
-
New Jersey Department of Health – Oral Health Services: Lists resources and community programs. NJ DOH Oral Health
-
NJDA Access to Care Program: The New Jersey Dental Association’s resource for patients seeking access to care. NJDA Foundation
-
Dental Lifeline Network – New Jersey: Provides comprehensive dental treatment for people who are elderly, disabled, or medically fragile. Dental Lifeline Network
-
Local Federally Qualified Health Centers (FQHCs): Offer sliding-scale fees based on income. Use the HRSA Find a Health Center tool: https://findahealthcenter.hrsa.gov/
Disclaimer: This article is for informational purposes only and does not constitute medical or financial advice. Individual circumstances vary greatly. Always consult with a qualified dental professional for diagnosis and treatment planning, and with a financial advisor for guidance on costs and insurance. The author and publisher are not liable for any decisions made based on this content.
Date: December 03, 2025
Author: The Dental Health & Economics Research Group