ADA Code for Cosmetic Bonding: A Complete Guide for Dental Professionals
Let’s be honest for a second. Dental coding can feel like a maze. You have a patient sitting in your chair. They want a small chip on their front tooth fixed. It is clearly a cosmetic issue. But your front desk team needs a code to bill. And the patient wants to know if their insurance will help.
You have probably asked yourself: What is the exact ADA code for cosmetic bonding?
The short answer is that cosmetic bonding does not have a unique, standalone ADA code labeled “cosmetic.” Instead, dentists use the same procedure codes for restorative bonding. The difference comes down to how you document the service, where you place the restoration, and the patient’s insurance plan.
In this guide, we will walk through everything you need to know. We will cover the correct codes, when to use them, how to handle insurance rejections, and practical tips for your dental practice. No fluff. No fake information. Just honest, real-world advice.
Let’s dive in.
What Is Cosmetic Bonding in Dentistry?
Before we talk about codes, let us quickly define what cosmetic bonding means in a clinical setting.
Cosmetic bonding, also known as direct composite bonding, involves applying a tooth-colored resin material to a tooth. The dentist sculpts, shapes, and polishes the resin. The goal is to improve the tooth’s appearance. Common uses include:
-
Repairing chipped teeth
-
Closing small gaps between teeth (diastemas)
-
Changing the shape of a tooth
-
Covering discoloration that whitening cannot fix
-
Protecting a worn tooth edge
Unlike veneers or crowns, bonding is usually done in one visit. It is less expensive and less invasive. But it is also less durable.
From a coding perspective, the procedure is identical to a standard composite restoration. The difference is the reason for doing it. That reason affects how insurance companies view the claim.
Important note: Insurance companies do not pay for cosmetic procedures in most cases. However, if the bonding also restores function or structure, you may have a case for reimbursement. We will explain how to do this correctly later.
The Primary ADA Code for Cosmetic Bonding
The most common ADA code for cosmetic bonding is D2330. But wait. There is more to the story.
D2330 specifically means: Resin-based composite crown, anterior, permanent tooth.
However, that code only applies to the front teeth (incisors and canines). If you are bonding a premolar or molar, you will use a different code.
Let us break down all the relevant codes in a clear table.
Table 1: ADA Codes for Composite Bonding (Anterior and Posterior)
| ADA Code | Description | Tooth Location | Typical Use for Cosmetic Bonding |
|---|---|---|---|
| D2330 | Resin-based composite crown, anterior, permanent tooth | Front teeth (incisors/canines) | Full coverage bonding for chips, shape changes, or gaps |
| D2331 | Resin-based composite, anterior, 1 surface | Front teeth | Small chip repair on one surface (facial or incisal) |
| D2332 | Resin-based composite, anterior, 2 surfaces | Front teeth | Chip involving two surfaces (e.g., facial and incisal) |
| D2335 | Resin-based composite, anterior, 3 or more surfaces | Front teeth | Larger bonding involving multiple tooth surfaces |
| D2391 | Resin-based composite, posterior, 1 surface | Premolars/molars | Small cosmetic reshaping of a back tooth (rare but possible) |
| D2392 | Resin-based composite, posterior, 2 surfaces | Premolars/molars | Cosmetic contouring involving two surfaces |
| D2393 | Resin-based composite, posterior, 3 surfaces | Premolars/molars | Larger cosmetic restoration on a back tooth |
| D2394 | Resin-based composite, posterior, 4 or more surfaces | Premolars/molars | Full cosmetic coverage on a posterior tooth |
As you can see, the ADA code for cosmetic bonding is not one single number. It depends on the tooth and the number of surfaces involved.
Which Code Should You Use Most Often?
For a typical small chip on a front tooth, most dentists use D2331 (one surface) or D2332 (two surfaces). For a gap closure or a full reshaping, D2330 is more appropriate.
Here is a simple rule of thumb:
-
One small chip on the edge of a front tooth → D2331
-
A chip on the edge plus the front surface → D2332
-
Closing a gap between two front teeth → D2330 (often billed per tooth)
-
Changing the shape of a tooth completely → D2330
Always document the surfaces you treat. For example: facial (F), incisal (I), mesial (M), distal (D). Good documentation protects you during an audit.
Why Insurance Usually Denies Cosmetic Bonding
Let’s be realistic. Most dental insurance plans exclude cosmetic procedures. The keyword here is cosmetic. If you submit a claim with a diagnosis code that only describes appearance, the payer will deny it.
However, there is a gray area. Many bonding procedures have both cosmetic and functional benefits.
For example:
-
A chipped incisal edge affects biting. That is functional.
-
A worn tooth from grinding needs protection. That is functional.
-
A gap that traps food can lead to decay. That is functional.
If you can show medical or dental necessity, some plans will cover part of the procedure.
Table 2: Cosmetic vs. Functional Reasons for Bonding
| Clinical Situation | Purely Cosmetic? | Functional Component? | Likely Insurance Coverage |
|---|---|---|---|
| Small chip with no pain or sensitivity | Yes | No | Denied |
| Deep chip exposing dentin (sensitivity) | No | Yes | Partial coverage possible |
| Gap between teeth (diastema) with no food trapping | Yes | No | Denied |
| Gap that traps food and causes inflammation | No | Yes | Possible coverage |
| Worn edge from bruxism | No | Yes | Often covered (under parafunction) |
| Discolored tooth from tetracycline | Yes | No | Denied |
| Fractured tooth from trauma | No | Yes | Usually covered (medical may apply) |
The takeaway? Do not assume bonding is always cosmetic. Trauma, wear, and sensitivity change the picture.
How to Document Cosmetic Bonding for Better Reimbursement
Documentation is your best friend. If you want to avoid denials, you need to write clear, honest notes. Do not exaggerate. Do not invent symptoms. But do not understate the functional need either.
Here is a checklist for your clinical notes when performing bonding:
-
Tooth number and surfaces treated (e.g., tooth #8, facial and incisal)
-
Reason for treatment (e.g., “Patient reports sensitivity to cold on #8 due to chipped incisal edge exposing dentin.”)
-
Pre-op condition (e.g., “Sharp edge noted. Patient caught lip on the edge twice last week.”)
-
Intraoral photos (attach if possible)
-
Diagnostic codes (ICD-10) that support medical necessity
-
Informed consent (including cosmetic limitations if insurance denies)
Recommended ICD-10 Codes to Pair with Bonding
| Condition | ICD-10 Code | Description |
|---|---|---|
| Chipped tooth due to trauma | S02.5XXA | Fracture of tooth (initial encounter) |
| Worn tooth from bruxism | F45.8 | Other somatoform disorders (bruxism) or K03.1 (attrition of teeth) |
| Tooth sensitivity | K08.89 | Other specified disorders of teeth |
| Fracture with pulp exposure | S02.5 | Use appropriate 7th character |
| Diastema with food impaction | K08.9 | Disorder of teeth, unspecified (weaker, but sometimes accepted) |
Important: Do not use trauma codes if there was no trauma. Insurance fraud is a serious offense. Always document what actually happened.
Step-by-Step: Submitting a Claim for Cosmetic Bonding
When your front desk team submits the claim, they need to follow a specific workflow. Let’s walk through it.
Step 1: Choose the Correct ADA Code
Use the table above. Match the tooth location and surface count.
Step 2: Add the Right ICD-10 Code
If the patient has sensitivity, use K08.89. If they have a fracture from biting something hard, use S02.5XXA. If it is purely cosmetic, use Z41.8 (encounter for other specified cosmetic procedures). But know that Z41.8 will almost always result in a denial.
Step 3: Write a Clear Narrative
Most electronic claim forms have a “remarks” or “narrative” field. Use it. Write one or two sentences explaining why the bonding is not purely cosmetic.
Example: “Tooth #8 incisal edge fracture extends into dentin. Patient reports sharp pain to cold air. Restoration restores contour and protects pulp.”
Step 4: Attach Supporting Documentation
If the claim is for a larger amount, consider attaching a pre-treatment estimate (prior authorization). This costs you time but saves frustration later.
Step 5: Submit and Track
Submit electronically. Note the date. If you do not hear back in 30 days, follow up.
What to Do When Insurance Denies Cosmetic Bonding
Denials are common. Do not get frustrated. You have options.
Option 1: Appeal with Clinical Notes
Send a formal appeal letter. Include:
-
A copy of your original claim
-
The denial letter from the payer
-
Your clinical notes highlighting functional necessity
-
Intraoral photos (if available)
-
A short narrative from the patient describing symptoms (e.g., “I cannot bite into an apple.”)
Option 2: Bill the Patient Directly
If the denial stands, you can bill the patient. Just make sure they signed a waiver before treatment. The waiver should say: “I understand that my insurance may deny this procedure as cosmetic. I am responsible for all fees regardless of insurance determination.”
Option 3: Adjust Your Fee
Some practices offer a “cash discount” for cosmetic bonding. This is legal as long as you do not commit insurance fraud (e.g., billing insurance and waiving the copay without adjusting the claim).
Option 4: Recommend Alternative Procedures
If the patient wants coverage, bonding may not be the answer. A resin-based composite done for structural reasons (e.g., replacing an old filling) is often covered. Or a crown for a fractured cusp. Discuss alternatives.
Cosmetic Bonding vs. Other Procedures: A Cost and Coverage Comparison
Patients often confuse bonding with other cosmetic treatments. Here is a quick comparison table to help you explain the differences.
Table 3: Bonding vs. Veneers vs. Crowns vs. Whitening
| Procedure | ADA Code(s) | Average Cost (per tooth) | Insurance Coverage | Longevity |
|---|---|---|---|---|
| Cosmetic bonding (composite) | D2330–D2335 | $300 – $600 | Rarely (unless functional) | 3–7 years |
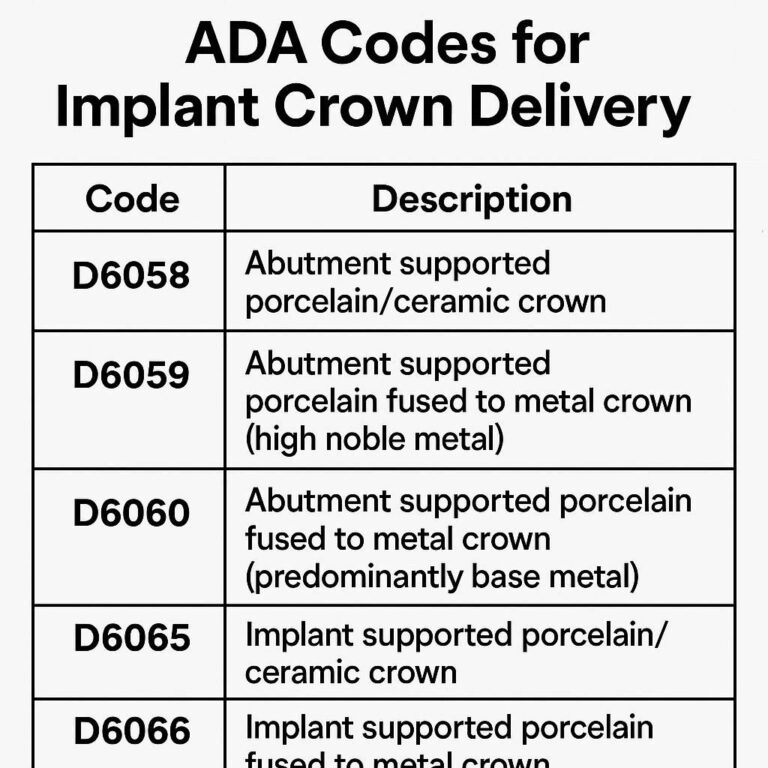
| Porcelain veneer | D2960–D2962 | $1,000 – $2,500 | Almost never | 10–15 years |
| Full crown (porcelain/ceramic) | D2740 | $1,200 – $3,000 | Often (if structural need) | 10–15+ years |
| Professional whitening | D9975 | $300 – $800 | Never (elective) | 1–3 years |
As you can see, bonding is the most affordable cosmetic option. But it is also the least durable and least likely to be covered.
Real-World Scenarios: Coding Examples
Let us walk through three common patient cases. Each case shows how to choose the correct ADA code for cosmetic bonding.
Case 1: Small Chip, No Sensitivity
-
Patient: 28-year-old female
-
Issue: Tiny chip on the incisal edge of tooth #9. No pain. No sharp edge.
-
Patient goal: “I just want it to look normal.”
-
ADA code: D2331 (anterior, 1 surface)
-
ICD-10: Z41.8 (cosmetic procedure)
-
Likely insurance outcome: Denied. Patient pays full fee.
Case 2: Moderate Chip with Sensitivity
-
Patient: 45-year-old male
-
Issue: Chipped tooth #8 after biting a popcorn kernel. Sharp edge. Pain with cold drinks for two weeks.
-
Patient goal: “It hurts and looks bad.”
-
ADA code: D2332 (anterior, 2 surfaces – facial and incisal)
-
ICD-10: S02.5XXA (fracture of tooth, initial encounter) + K08.89 (sensitivity)
-
Likely insurance outcome: Partial coverage after appeal (50–80% of D2332 fee).
Case 3: Closing a Gap Between Two Front Teeth
-
Patient: 22-year-old male
-
Issue: 1.5mm diastema between teeth #8 and #9. No food trapping. No pain.
-
Patient goal: “I hate the gap. It looks unprofessional.”
-
ADA code: D2330 (resin crown, anterior) on each tooth (two units)
-
ICD-10: Z41.8
-
Likely insurance outcome: Denied. Patient pays in full.
Ethical Considerations for Billing Cosmetic Bonding
This section is important. Do not skip it.
Bonding is a wonderful procedure. Patients love the instant results. But as a dental professional, you have an ethical duty to bill honestly.
-
Do not upcode. If you did a one-surface bonding, do not bill a three-surface code.
-
Do not fabricate trauma. If the chip is old and asymptomatic, do not use an S02.5 code.
-
Do not guarantee insurance coverage. Tell patients upfront: “Your plan may consider this cosmetic. You are responsible for the fee if they deny.”
Transparency builds trust. Trust brings repeat patients and referrals.
“I always tell my patients before starting cosmetic bonding: assume your insurance will say no. If they say yes, that is a bonus. This sets the right expectation from the start.” — Dr. Elena R., general dentist, Austin, TX
How to Explain ADA Codes to Your Patients
Patients do not understand dental coding. And they should not have to. But you can help them by using plain language.
Instead of saying: “We will use D2331 for the composite on #8,” try this:
*“We are going to repair the chip on your front tooth using a tooth-colored filling. The technical code for this is D2331. It means we are working on one surface of your front tooth. I want you to know that insurance often calls this cosmetic, so you might get a bill for the full amount. Let me show you our financial policy.”*
This approach reduces confusion and prevents billing disputes later.
Common Mistakes Dentists Make with Cosmetic Bonding Codes
Avoid these errors. They cost you time and money.
Mistake 1: Using D2330 for Everything
D2330 is a crown. Not a small filling. If you only restore a small area, use a surface-specific code (D2331, D2332, D2335).
Mistake 2: Forgetting to Document Surfaces
Insurance auditors look for surface codes. If you write “composite #8” without specifying facial, incisal, etc., they may downcode or deny.
Mistake 3: Not Obtaining a Cosmetic Waiver
Always have a signed cosmetic waiver for any bonding where the primary goal is appearance. This protects you if the patient later refuses to pay.
Mistake 4: Assuming All Anterior Bonding Is Cosmetic
Some anterior bonding is restorative. For example, replacing an old, leaking composite filling on tooth #10 is a covered benefit under most plans. Do not automatically call it cosmetic.
Future Trends in Dental Coding for Cosmetic Bonding
The ADA updates its code set every year. While cosmetic bonding codes have not changed recently, there is ongoing discussion about creating a specific “direct cosmetic composite” code. However, as of 2026, no such code exists.
Insurance companies are also tightening rules. More plans now require pre-authorization for any anterior composite on teeth #6 through #11. Check each payer’s policy before treatment.
If you want to stay updated, bookmark the ADA’s official coding website. Link provided at the end of this article.
Frequently Asked Questions (FAQ)
1. Is there a specific ADA code just for cosmetic bonding?
No. Dentists use the same codes as restorative composite bonding (D2330–D2335 for anterior teeth, D2391–D2394 for posterior teeth). The difference is in the diagnosis code and documentation.
2. Will my insurance pay for cosmetic bonding?
Usually, no. Most dental plans exclude procedures done solely for appearance. However, if the bonding restores function (e.g., a fractured tooth with sensitivity), you may receive partial coverage.
3. What ADA code do I use for bonding a gap between front teeth?
Use D2330 (resin crown, anterior) for each tooth involved. Some dentists use D2335 if three or more surfaces require bonding.
4. Can I bill medical insurance for cosmetic bonding after trauma?
Yes, in some cases. If the trauma is acute (e.g., a fall or accident), medical insurance may cover the repair. Use a medical claim form (CMS-1500) with the appropriate ICD-10 trauma code.
5. What is the difference between D2331 and D2332?
D2331 is for one surface (e.g., just the facial surface). D2332 is for two surfaces (e.g., facial and incisal, or mesial and facial). Choose based on how many tooth surfaces you actually treat.
6. How long does cosmetic bonding last?
Typically 3 to 7 years, depending on oral habits, location, and maintenance. Front tooth bonding lasts longer if the patient avoids biting hard objects.
7. Do I need to send X-rays with a bonding claim?
For single-surface bonding, no. For D2330 (resin crown) or multi-surface codes, some payers request a post-treatment bitewing to confirm the restoration. Check each plan’s medical necessity guidelines.
8. What happens if I use the wrong ADA code?
The claim may be denied, delayed, or downcoded. In extreme cases, repeated incorrect coding can trigger an audit. Always double-check your codes.
Additional Resources
For the most current ADA codes, coding guidelines, and annual updates, visit the official American Dental Association Coding Center:
🔗 www.ada.org/en/publications/cdt
For insurance appeal letter templates and denial management tools, the American Association of Dental Office Management (AADOM) offers free resources for members:
🔗 www.aadom.org
Conclusion
The ADA code for cosmetic bonding is not a single number. It depends on the tooth location and the number of surfaces treated. For most front teeth, you will use D2331 (one surface), D2332 (two surfaces), or D2330 (full resin crown). Insurance rarely covers purely cosmetic bonding, but functional needs like trauma, sensitivity, or wear can justify coverage with proper documentation. Always be honest, obtain a signed cosmetic waiver, and explain financial responsibility to patients before treatment.