ADA Codes for Implant Crown Delivery
So, you have just placed a beautiful implant, and now it is time for the moment every dentist and patient waits for: delivering the final crown.
But then comes the paperwork. You open your billing software and stare at a list of codes that all look somewhat similar. Do you use D6058? Or is it D6062? Maybe D6066?
You are not alone. Implant coding is one of the most confusing areas in dental billing. The American Dental Association (ADA) has created specific codes for implant crown delivery, but they change based on the type of restoration, the material, and how the crown attaches to the abutment.
This guide will walk you through every relevant ADA code for implant crown delivery. No fluff. No copied definitions. Just clear, honest explanations that help you bill correctly and get paid fairly for your work.
Let us clear up the confusion together.
Why the Right ADA Code Matters for Implant Crowns
Using the wrong code is not just a clerical error. It can lead to claim denials, delayed payments, and even audits. Insurance companies are paying close attention to implant codes because these procedures cost more than traditional crowns.
When you deliver an implant crown, you are not just cementing a cap. You are restoring function and aesthetics over a dental implant. The code you choose tells the insurance story:
-
What type of abutment did you use?
-
Is the crown screw-retained or cemented?
-
Did you provide the abutment separately?
Getting this right means fewer phone calls with insurance adjusters. It means faster reimbursement. And most importantly, it means you can focus on your patients instead of fighting with paperwork.
The Main ADA Code for Implant Crown Delivery: D6058
Let us start with the most common code you will use.
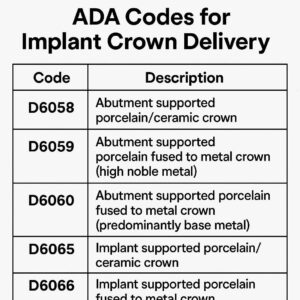
D6058 is defined by the ADA as “Abutment supported porcelain/ceramic crown.”
In plain English, this code covers a crown that is made entirely of porcelain or ceramic and is placed on an abutment that is already attached to the implant. This is your standard, go-to code for delivering a full-ceramic implant crown.
When do you use D6058? Imagine this scenario. You have placed a healing abutment. The tissue has matured. You remove the healing abutment and place a stock abutment or a custom abutment. Then, you deliver a beautiful zirconia crown that cements onto that abutment. That is D6058.
What D6058 Includes
This code assumes you are providing both the abutment and the crown. It covers the crown itself, the chairtime for delivery, and the adjustments needed to make sure the bite feels right.
What D6058 Does Not Include
This code does not cover the implant body placement. That is a separate code (D6010). It also does not cover the surgical guide or any bone grafting. Those have their own codes.
D6059: The Metal Alternative
Not every patient wants porcelain. Some back teeth need the strength of metal. For those cases, you will use D6059 – “Abutment supported cast metal crown.”
This code is identical to D6058 in every way except for the material. The crown is made entirely of cast metal, usually a high-noble alloy. You see these less often today, but they are still excellent for patients with heavy bites or limited interocclusal space.
A Quick Comparison of D6058 and D6059
| Feature | D6058 | D6059 |
|---|---|---|
| Material | Porcelain or ceramic | Cast metal (alloy) |
| Aesthetics | Excellent | Poor |
| Strength | Good | Excellent |
| Typical use | Anterior or premolar | Molar |
| Lab fee | Moderate | Lower |
D6062: When Metal Meets Porcelain
Some patients want the strength of metal with the look of porcelain. That is where D6062 comes in. This code is for “Abutment supported porcelain fused to metal crown.”
This is the classic PFM crown, but on an implant abutment. You might choose this code for a patient who needs the durability of a metal substructure but wants a tooth-colored appearance on the outside.
Many dentists are moving away from PFM for implants because of the risk of porcelain chipping. However, for long-span bridges or patients with very heavy forces, D6062 remains a solid choice.
D6063: The Economical Choice
Not every crown needs to be high-end. For temporary restorations or cases where budget is a major concern, you have D6063 – “Abutment supported resin crown.”
This is a crown made of acrylic or composite resin. It is much weaker than ceramic or metal. You would rarely use this as a permanent delivery code. Instead, you might use D6063 for a provisional crown while the lab fabricates the final restoration.
Some insurance plans cover resin crowns for implant restorations in specific situations, such as for patients with severe bruxism who will break anything stronger. But always check your patient’s benefits first.
Screw-Retained vs. Cemented: The Big Decision
Now things get a little more complex. The codes above are all for crowns that cement onto an abutment. But what if you want to screw the crown directly to the implant?
The ADA has separate codes for screw-retained implant crowns. These are becoming more popular because they are retrievable. If something breaks, you can unscrew the crown instead of cutting it off.
Here are the codes you need for screw-retained delivery.
D6066: The Modern Favorite
D6066 is defined as “Implant supported crown – porcelain/ceramic.”
Pay close attention here. D6066 does not mention an abutment. That is because the crown itself is designed to screw directly into the implant. The crown has a small screw hole that you cover with composite after tightening.
This code is exploding in popularity. Many implant companies now make one-piece screw-retained crowns that are strong, beautiful, and easy to repair. If you are placing a posterior crown and want retrievability, D6066 is your best friend.
D6067: Metal Screw-Retained Crown
For the metal version of a screw-retained crown, use D6067 – “Implant supported crown – cast metal.”
This is rare today. But if a patient needs a pure metal crown for a lower second molar and you want to screw it directly to the implant, this is the correct code.
D6068: PFM Screw-Retained Crown
Finally, D6068 covers “Implant supported crown – porcelain fused to metal.” This is a screw-retained PFM crown. You will see this code used more often in older treatment plans or in countries where PFM is still the standard.
A Helpful List: Cemented vs. Screw-Retained Codes
Here is a simple breakdown to keep at your desk.
Cemented onto an abutment:
-
D6058 – Porcelain/ceramic crown
-
D6059 – Cast metal crown
-
D6062 – PFM crown
-
D6063 – Resin crown
Screw-retained directly to the implant:
-
D6066 – Porcelain/ceramic crown
-
D6067 – Cast metal crown
-
D6068 – PFM crown
Important Note for Readers: Some insurance plans do not recognize screw-retained codes yet. They may ask you to use the cemented codes instead. Always call the insurance company before submitting a claim for D6066 if you are unsure. Honest communication saves headaches later.
The Abutment Puzzle: Do You Bill Separately?
This is where many claims go wrong.
The codes above (D6058 to D6068) include the abutment. That is right. When you bill D6058, you are telling the insurance company that the price covers both the abutment and the crown.
But what if the patient already has an abutment from a previous procedure? Or what if you place a custom abutment that costs more than a stock abutment?
In those cases, you might bill the abutment separately using D6057 (custom abutment) or D6056 (prefabricated abutment). Then, you would bill the crown code with a modifier that indicates the abutment was already provided.
However, this is tricky. Most insurance companies expect a single code that includes everything. Separating them can trigger a denial. My honest advice? Unless you are billing a fee-for-service patient or you have written pre-approval from the insurance plan, stick with the single code.
Step-by-Step: How to Choose the Right Code for Delivery Day
Let us walk through a real appointment. Your patient is in the chair. The implant is osseointegrated. You are ready to deliver the final crown.
Step 1: Identify the abutment situation.
-
Are you placing a new abutment today? Move to step 2.
-
Does the patient already have an abutment from a prior visit? You may need a different code or a modifier.
Step 2: Decide on retention.
-
Will the crown cement onto the abutment? Use D6058, D6059, D6062, or D6063.
-
Will the crown screw directly into the implant? Use D6066, D6067, or D6068.
Step 3: Choose the material.
-
Full ceramic (zirconia, lithium disilicate) → D6058 or D6066.
-
Metal only → D6059 or D6067.
-
PFM → D6062 or D6068.
-
Temporary resin → D6063.
Step 4: Check the insurance plan.
-
Does the plan cover implant crowns? Many do not.
-
Does the plan have a missing tooth clause? If the tooth was missing before the policy started, they may deny coverage.
-
Does the plan require a pre-authorization? If yes, use the same code you got approved.
Step 5: Document everything.
Take a periapical X-ray of the seated crown. Write a detailed narrative. Note the implant system, the torque value used, and the patient’s bite confirmation. This documentation is your shield against audits.
Common Mistakes to Avoid During Billing
Even experienced dentists mess these up. Here are the most frequent errors I see.
Mistake 1: Using a traditional crown code (D2740).
A traditional crown goes on a natural tooth. An implant crown goes on an abutment or implant. They are not the same. D2740 on an implant claim will get rejected every time.
Mistake 2: Forgetting the abutment code.
If you use a code like D6058, you are fine. But if you try to bill the crown and abutment separately without a modifier, the insurance company may pay for only one of them.
Mistake 3: Billing for the crown before the implant is ready.
Some dentists try to submit the crown code on the same day as the implant placement. Do not do this. The crown delivery happens months later. Separate the dates.
Mistake 4: Not using the right number of surfaces.
Implant crowns are almost always coded as “full crowns.” You do not need to specify surfaces like you do with a three-quarter crown on a natural tooth.
A Realistic Look at Insurance Reimbursement
Let me be honest with you. Many dental insurance plans do not cover implant crowns at all. They consider implants a “cosmetic” or “major” procedure with low annual maximums.
When they do cover implant crowns, the reimbursement is often low. You might see a plan that pays $500 for a crown that costs you $300 in lab fees plus chairtime. That leaves very little profit.
This is why many dentists bill implant crowns as fee-for-service. You present the treatment plan, the patient pays you directly, and you help them submit their own insurance claim for out-of-network reimbursement.
If you choose to stay in-network, read your contract carefully. Some PPO plans will downgrade an implant crown to a traditional crown benefit. Others will deny it entirely.
Quotation from a billing expert: “The most successful implant practices do not rely on insurance to pay for the crown. They present the value of the restoration and collect payment upfront. Then they treat insurance reimbursement as a bonus, not a necessity.” – Sarah J., Dental Billing Consultant.
How to Write a Bulletproof Claim Narrative
Your claim needs more than just a code. It needs a story. Insurance adjusters read hundreds of claims per day. A weak narrative gets denied. A strong narrative gets paid.
Here is a template you can adapt.
*”Patient presented for delivery of final implant crown. Implant body (D6010) was placed on [date] and confirmed osseointegrated via periapical radiograph. A [stock/custom] abutment was torqued to [value] Ncm. The final [material] crown (D6058) was seated, adjusted for occlusion, and cemented with [cement name]. Post-operative radiograph confirms complete seating. Patient tolerated procedure well.”*
Add the implant brand, the lot number of the abutment if available, and any warranty information. More detail is better.
ADA Codes for Related Procedures on Delivery Day
Delivering an implant crown sometimes involves extra steps. Here are other codes you might use on the same day.
D6011 – Second-stage implant surgery. Use this if you need to uncover a submerged implant before placing the abutment.
D6056 – Prefabricated abutment. Use this if you are placing a stock abutment and billing it separately from the crown. But remember the warning above about separate billing.
D6057 – Custom abutment. Use this for a lab-fabricated abutment. These are more expensive and usually billed separately in fee-for-service practices.
D6092 – Recementing an implant crown. If a patient comes back with a loose crown, this is the code. Do not use a traditional recement code.
D6095 – Repair of an implant crown. Small chip? Use this code. Large fracture usually needs a new crown.
The Future of Implant Crown Coding
The ADA updates its CDT codes every year. In recent years, we have seen more clarity around digital workflows and same-day crowns.
There is talk of creating separate codes for same-day milled implant crowns versus lab-fabricated crowns. As of this writing, no such distinction exists. But watch for changes. The world of digital dentistry moves fast.
For now, the codes above remain the standard. Focus on mastering D6058 and D6066. Those two codes will cover 80% of your implant crown deliveries.
Frequently Asked Questions (FAQ)
Q1: Can I use D2740 for an implant crown?
No. D2740 is for a crown on a natural tooth. Using it for an implant crown is incorrect and will likely result in a denial or an audit.
Q2: What is the difference between D6058 and D6066?
D6058 is a cemented crown on an abutment. D6066 is a screw-retained crown that attaches directly to the implant. D6066 has a screw hole that you fill with composite.
Q3: Does insurance cover D6066 the same as D6058?
Not always. Some plans do not recognize screw-retained codes yet. Always verify with the specific insurance company before treatment.
Q4: Can I bill for the abutment and the crown separately?
Yes, but only in specific situations, such as when a patient already has an abutment from a prior procedure. For most deliveries, a single code like D6058 includes both.
Q5: What code do I use for a temporary implant crown?
Use D6063 for a resin temporary crown on an abutment. For a screw-retained temporary, check if your implant system has a specific provisional code. Some offices use D6094 for a crown removal and temporary.
Q6: How do I code a same-day cerec implant crown?
Use the same codes as a lab crown. If you mill a ceramic crown and cement it to an abutment, use D6058. If you screw it directly, use D6066. The fabrication method does not change the code.
Q7: What if the patient loses the crown?
A replacement crown is not a “delivery” of the original. Use D6092 for recementing if the crown is intact. If the crown is lost or broken beyond repair, you may need to bill a new crown code. Check your patient agreement first.
Q8: Do I need to submit an X-ray with the claim?
Most plans do not require an X-ray for a crown delivery claim, but they may ask for it later. Attach a post-delivery periapical X-ray to the claim if your software allows it. This prevents delays.
Additional Resources
For the most current ADA CDT codes and official definitions, always refer directly to the American Dental Association’s website.
Link: Visit the ADA’s official CDT Code page
(This link leads to the official source for dental coding. Always verify codes there before submitting a claim.)
A Final Word on Honesty and Ethics
Do not manipulate codes to get better reimbursement. Do not bill D6058 when you placed a resin temporary. Do not bill an implant crown as a bridge abutment. These shortcuts may work once or twice, but audits are real. When they happen, they are not friendly.
Be honest. Document well. Charge a fair fee for your skill and materials. Your patients will appreciate your transparency, and your reputation will grow stronger than any short-term gain from creative billing.
Conclusion
Delivering an implant crown is a rewarding procedure that restores both function and confidence. The ADA code you choose tells the story of that restoration. For most cemented ceramic crowns on an abutment, D6058 is your answer. For screw-retained restorations, turn to D6066. Match the code to the material and retention method, document thoroughly, and bill honestly. This approach keeps your claims clean, your payments predictable, and your focus where it belongs: on your patients.