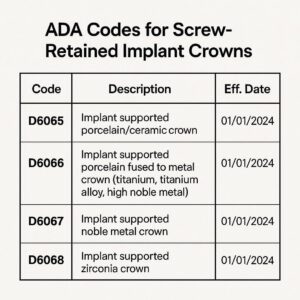
ADA Codes for Screw-Retained Implant Crowns
If you are a dentist, a treatment coordinator, or a billing specialist, you know that the world of dental implant coding can sometimes feel like navigating a maze. You have the clinical skills to place a beautiful, functional screw-retained crown, but when it comes time to translate that work into a billing code, things can get confusing.
The American Dental Association (ADA) maintains the Current Dental Terminology (CDT) codes. These are the language we use to communicate with insurance companies. For a procedure as specific as a screw-retained implant crown, using the right code is not just about getting paid; it is about maintaining accurate patient records and avoiding audits.
This guide is designed to be your friendly, reliable companion through that process. We will break down the specific codes, explain when to use them, and clarify the nuances that often lead to claim denials. Whether you are new to implant dentistry or a seasoned pro looking for a refresher, you will find practical, realistic advice here.
Let’s get started.
Understanding the Basics: Implant Restoration vs. Natural Tooth
Before we dive into the specific codes, we need to establish a fundamental principle in dental coding. Insurance companies and the ADA treat restorations supported by implants very differently than those supported by natural teeth.
When you restore a natural tooth with a crown, you are usually looking at codes in the D2700 – D2799 series (like D2740 for porcelain crown). However, when you are placing a crown on an implant, you are dealing with a prosthesis. It is a different category entirely.
A screw-retained implant crown is a prosthesis that attaches directly to the implant abutment (or the implant itself) via a screw. Because there is no cement, the retrievability factor is high. From a coding perspective, we focus on the connection and the restoration of the implant.
Why Coding Matters
Accurate coding protects your practice. If you use a standard crown code for an implant crown, the insurance company may deny the claim outright, or worse, pay a lower fee that doesn’t reflect the complexity of the implant restoration. More importantly, accurate coding ensures that the patient’s lifetime maximum benefits are applied correctly to the right procedures.
The Primary ADA Codes for Screw-Retained Implant Crowns
When we talk about a screw-retained implant crown, we are typically looking at two main codes, and occasionally a third. The choice depends on whether you are using a stock abutment, a custom abutment, or a screw-retained crown that attaches directly to the implant.
Let’s break these down.
D6058: Abutment Supported Porcelain/Ceramic Crown
This is often the most common code used for a screw-retained crown, but it requires a specific context. Code D6058 is defined as a “prefabricated abutment – porcelain/ceramic crown.”
In simple terms, this code is used when you are placing a porcelain or ceramic crown onto a prefabricated (stock) abutment.
-
The Scenario: You have placed the implant. It has osseointegrated. You select a stock titanium or zirconia abutment from a catalog (like a straight or angled stock abutment). You screw that abutment into the implant. Then, you fabricate a crown that is cemented onto that abutment.
-
Wait, is that screw-retained? In this scenario, the crown is cement-retained onto the abutment, but the abutment is screw-retained to the implant.
-
The Confusion: Many clinicians use this code for screw-retained restorations, but technically, the crown itself is cement-retained if an abutment is involved.
However, what if the crown is fabricated as a single unit with the abutment? That brings us to our next code.
D6060: Implant Supported Crown
This code is often used when the restoration is a single, screw-retained unit where the crown and abutment are one piece, or when the crown is directly screwed into the implant without a separate abutment.
Code D6060 is defined as “implant supported crown – porcelain/ceramic.”
-
The Scenario: This is your true “screw-retained” crown. In this case, the technician fabricates a single unit that combines the abutment and the crown. There is no cement involved. The entire restoration is torqued down through a screw channel in the occlusal surface directly into the implant fixture.
-
Why use this? This code is more accurate for a monolithic screw-retained crown because it describes the restoration as being supported directly by the implant, without a separate cementable interface.
D6057: Custom Abutment
Sometimes, you cannot use a stock abutment. The angle is off, the depth is tricky, or you simply need a highly customized emergence profile. In these cases, you fabricate a custom abutment.
Code D6057 is used for the “custom fabricated abutment.” This is often billed in addition to the crown code.
-
The Scenario: You need a custom milled or cast abutment to create the ideal emergence profile and angulation for the final crown. You bill D6057 for the abutment. Then, you bill either D6058 (if you are cementing a crown onto that custom abutment) or D6060 (if you are creating a screw-retained unit on top of that custom abutment).
A Quick Comparison Table
| ADA Code | Description | Typical Use Case | Screw-Retained? |
|---|---|---|---|
| D6058 | Abutment Supported Crown | Crown cemented onto a prefabricated (stock) abutment. | The abutment is screw-retained; the crown is cement-retained. |
| D6060 | Implant Supported Crown | A single unit crown that screws directly into the implant. | Fully screw-retained. No cement. |
| D6057 | Custom Abutment | A milled or cast abutment used to support a crown. | This is the abutment code. The final crown (D6058) sits on it. |
The Nuances: Screw-Retained vs. Cement-Retained
One of the biggest debates in implant dentistry is whether to code a restoration as “abutment supported” or “implant supported.” The insurance payer’s perspective is often different from the clinician’s.
If you are placing a crown that is fully screw-retained (the crown and abutment are one piece), your most accurate code is usually D6060.
If you are placing a cement-retained crown on a separate abutment (whether stock or custom), you will likely use D6058 (and D6057 if the abutment is custom).
Why Does This Distinction Matter?
Insurance companies often have different fee schedules for these codes. Sometimes, D6060 (implant supported crown) reimburses at a higher rate than D6058 because it implies a more complex laboratory process (the combined abutment/crown unit).
However, some payers view D6060 as a “screw-retained only” code. If you use D6060 and the insurance company reviews your X-ray and sees a separate abutment (cement-retained), they may downcode the claim to D6058 or deny it for incorrect coding.
Important Note: Always check the patient’s specific insurance policy. Some plans have a “missing tooth clause” or explicitly exclude implant restorations. Coding correctly will not override a plan exclusion, but it ensures that if the benefit exists, you are positioned to receive it.
Step-by-Step: Building Your Claim for a Screw-Retained Crown
Let’s walk through a typical clinical scenario to see how these codes come together on a claim form.
Scenario: A patient needs a single screw-retained implant crown on tooth #19. The implant is already placed and healed (we are only dealing with the restoration phase). The doctor decides to use a custom abutment to correct a slight buccal angulation, and the lab fabricates a screw-retained crown that fits on top of that custom abutment.
Here is how you would build your claim:
-
Code: D6057 (Custom Abutment)
-
Description: Fabrication and placement of a custom abutment.
-
Date: The date the abutment was delivered and torqued.
-
-
Code: D6058 (Abutment Supported Crown)
-
Description: Porcelain/ceramic crown placed on the custom abutment.
-
Date: The date the final crown was seated.
-
Alternative Scenario: The doctor uses a stock titanium abutment and cements a crown onto it.
-
Code: D6058 (Abutment Supported Crown)
-
Description: Porcelain/ceramic crown placed on a prefabricated abutment.
-
Alternative Scenario: The doctor places a screw-retained crown that attaches directly to the implant (no separate abutment).
-
Code: D6060 (Implant Supported Crown)
-
Description: Single unit screw-retained crown.
-
The “Abutment Connection” Code: D6056
There is a code that often gets confused with these: D6056 (Prefabricated Abutment). This code is used to bill for the stock abutment itself.
-
If you use a stock abutment, you may bill D6056 for the component, and D6058 for the crown.
-
However, some insurance companies consider D6056 to be “bundled” into the crown code (D6058). They view the stock abutment as part of the crown delivery procedure.
-
Conversely, D6057 (custom abutment) is almost always billed separately because it involves significant laboratory and chairside time.
Common Mistakes and How to Avoid Them
Even experienced billers can stumble on implant codes. Here are the most frequent errors we see with screw-retained crowns, along with solutions.
Mistake 1: Using Natural Tooth Crown Codes (D2740)
This is the most common error. D2740 is for a crown on a natural tooth. Using this for an implant restoration is incorrect. The insurance company will often reject it, stating that the tooth number provided is not a natural tooth (if they have records of the extraction) or that the code does not match the “implant” designation in the narrative.
Solution: Always use the D6000 series for implant restorations.
Mistake 2: Confusing the Abutment Codes
New team members often bill D6056 (prefabricated abutment) when they meant to bill D6057 (custom abutment), or vice versa. The reimbursement difference can be substantial. A custom abutment requires more lab work and should be billed accordingly.
Solution: Verify with the doctor. Did they scan for a custom abutment, or did they use a “stock” abutment from a tray? Document this in the patient’s chart.
Mistake 3: Incorrect Tooth Numbers
Implants do not use the standard tooth numbering system in the same way natural teeth do. While you will still use the number of the site (e.g., #19, #8), insurance adjusters look for consistency. If the implant was placed months ago and you are now restoring it, ensure your narrative explains that you are restoring the existing implant at site #19.
Solution: Always include a clear narrative: “Restoration of previously placed implant at site #19 with a custom abutment and porcelain crown.”
Mistake 4: Forgetting the Narrative
In the age of digital claims, we often forget the power of a simple narrative. For implant cases, a narrative is your best friend. If the claim looks unusual or the codes are complex, a one-sentence explanation can prevent a denial.
Solution: Attach a narrative that says: “Implant restoration: Custom abutment (D6057) fabricated and placed. Final crown (D6058) cemented onto abutment. Implant placed on [date].”
Navigating Insurance Limitations
It would be irresponsible to write a guide on coding without addressing the reality of insurance limitations. Implant dentistry is often poorly covered by traditional dental insurance plans.
Here are a few realities to keep in mind:
-
The Missing Tooth Clause: Many PPO plans have a clause that states they will not cover a bridge or implant to replace a tooth that was missing before the patient’s coverage began. If the patient lost the tooth five years ago and just joined the plan, the implant crown may be denied.
-
Frequency Limitations: Most plans cover a crown (natural tooth) once every 5 to 7 years. For implant crowns, they often apply the same frequency limitation. However, the “clock” usually starts from the date of the last crown on that tooth. If the tooth was extracted and an implant placed, there is no previous crown, so this can be argued.
-
Implant vs. Crown Benefits: Some plans have a separate implant benefit (usually with a lower annual maximum). Others cover the crown but not the abutment, or cover the abutment but not the crown. You must verify benefits thoroughly before starting treatment.
Tips for Successful Pre-Authorizations
A pre-authorization (pre-determination) is your safety net. It is not a guarantee of payment, but it gives you a strong indication of how the plan will process the claim.
When submitting a pre-authorization for a screw-retained implant crown:
-
Include the radiograph. Show the implant in place.
-
List all codes. Include the implant restoration code (D6058 or D6060), the abutment code (if applicable), and any surgical codes if the implant is being placed at the same time.
-
Provide a clear narrative. State exactly what you plan to do.
-
Wait for the response. Review the explanation of benefits (EOB) from the pre-auth carefully. Look for denial reasons. If the plan states they “do not cover implants,” you need to have a financial discussion with the patient before proceeding.
A Note on Digital Workflows and Coding
Digital dentistry has changed how we fabricate screw-retained crowns. Whether you are using an intraoral scanner and milling in-house or sending a digital impression to an external lab, the coding remains the same. The method of fabrication does not change the ADA code.
However, the type of restoration does.
-
Screw-Retained Zirconia Crown: If you mill a full-contour zirconia crown that screws directly into the implant (no separate abutment), this is D6060.
-
Cement-Retained Zirconia Crown on a Titanium Base: Many modern workflows use a titanium base (ti-base) that acts as a prefabricated abutment. The zirconia crown is cemented to the ti-base, and the ti-base is screwed into the implant. Even though the crown is “cement-retained” to the base, the overall restoration is retrievable via screw. In this case, because you are using a prefabricated abutment (the ti-base), the appropriate code is usually D6058 (abutment supported crown), and you may bill D6056 for the ti-base if your payer does not bundle it.
Building a Checklist for Your Team
To make sure your team is on the same page, creating a simple checklist for implant restoration coding can save hours of appeals later.
Implant Restoration Coding Checklist
-
Verify Implant Placement Date: Ensure the implant has had adequate healing time (unless it is an immediate load case).
-
Confirm Restoration Type:
-
Is it a single unit screw-retained crown? (D6060)
-
Is it a crown cemented onto a custom abutment? (D6057 + D6058)
-
Is it a crown cemented onto a stock abutment? (D6058)
-
-
Check Insurance Benefits:
-
Does the plan cover implants?
-
Is there a missing tooth clause?
-
What is the patient’s remaining annual maximum?
-
-
Prepare the Claim:
-
Attach a periapical or panoramic radiograph.
-
Write a concise narrative (e.g., “Restoration of previously placed implant #3 with custom abutment and PFM crown.”)
-
List all codes in the correct order (usually abutment first, then crown).
-
-
Submit and Track: Follow up on the claim if payment is not received within 30 days.
Documentation Best Practices
In the world of audits, documentation is king. If an insurance company audits your implant cases, you need to have your paperwork in order. Here is what you should keep in your patient records for every screw-retained implant crown:
-
Surgical Notes (if you placed the implant): Date of placement, implant system, lot numbers, and any bone grafting performed.
-
Restorative Notes: Detailed notes on the abutment selection (custom or stock), the torque values used, and the type of cement (if used) or screw channel material.
-
Laboratory Prescription: A copy of the lab slip showing what was fabricated.
-
Radiographs: A pre-operative (pre-restoration) radiograph showing the implant, a radiograph with the abutment in place, and a post-cementation radiograph showing the final crown.
-
Consent Forms: Signed consent forms specifically mentioning the implant restoration and the costs involved.
Frequently Asked Questions (FAQ)
To wrap up this comprehensive guide, let’s address some of the most common questions we hear from dental teams regarding ADA codes for screw-retained implant crowns.
Q1: If I place a screw-retained crown that combines the abutment and crown, do I bill D6057 and D6060?
No. If the crown and abutment are a single unit, you do not bill a separate custom abutment code (D6057). The fabrication of the abutment portion is included in the implant-supported crown code (D6060). You only bill D6057 if the abutment is a separate piece from the crown.
Q2: Can I bill for the screw access hole filling material?
No. There is no specific ADA code for filling the screw access hole with cotton, Teflon tape, or composite resin. This is considered part of the crown delivery procedure and is included in the fee for the crown code (D6058 or D6060).
Q3: What is the difference between D6058 and D6060 in terms of reimbursement?
This varies entirely by insurance carrier. Some plans reimburse D6060 at a higher rate because it represents a more complex laboratory fabrication (a hybrid abutment/crown). Others reimburse them identically. The key is to use the code that accurately reflects the service provided, not the one that pays more.
Q4: My patient has a “dual-arch” or “implant” plan. How does that affect coding?
Some plans have specific implant riders. They may have a separate annual maximum specifically for implant services. In these cases, using the correct codes (D6058, D6060, D6057, D6056) is critical to ensuring the claim goes toward the correct pool of benefits (implant pool vs. basic services pool).
Q5: Do I need to include a modifier for the tooth number?
Yes. In the “tooth number” field on the ADA claim form, you always enter the tooth number being restored (e.g., 30, 14). Even though the tooth is missing, you are restoring the site of that tooth. For the ADA, this is standard practice.
Q6: What if the implant crown breaks? Is there a warranty code?
If the crown breaks within the practice’s warranty period (usually 1-5 years), you would typically redo the crown at no charge. From a coding perspective, if you have to replace it for a fee due to patient damage outside the warranty, you would use the same code (D6060 or D6058) with a “replacement” narrative. You cannot use a “repair” code (D6090) for a crown that is completely fractured; D6090 is usually reserved for repairing the abutment or crown margin.
Additional Resources
For those looking to dive deeper into the nuances of dental coding, the best resource is always the official Current Dental Terminology (CDT) Codebook, published annually by the American Dental Association. This book provides the official definitions and guidelines directly from the source.
Additionally, many state dental associations offer coding seminars specifically focused on implant billing. These workshops are invaluable because they often feature real-world case studies and interactions with insurance representatives.
For online reference, the ADA’s Center for Professional Success offers articles and guides on coding for members. It is a reliable, up-to-date source that reflects the latest changes in the CDT manual.
Conclusion
Navigating the ADA codes for screw-retained implant crowns requires a blend of clinical understanding and administrative precision. In summary, remember these three core principles: use D6060 for a fully screw-retained, single-unit crown; use D6058 for a crown cemented onto an abutment; and use D6057 for a custom abutment when the clinical situation demands it. Accurate coding, thorough documentation, and a clear understanding of your patient’s insurance plan are the pillars of a successful implant billing process. By mastering these distinctions, you ensure your practice is reimbursed fairly while providing the highest standard of care to your patients.