Decoding the ADA Dental Codes for Implants
If you have been told you need a dental implant, you have probably heard a mix of terms that sound more like a science experiment than a medical procedure. “Abutment,” “fixture,” “crown.” Then, your dentist’s front desk hands you a treatment plan filled with five-digit codes and numbers that seem to have no relation to the actual tooth you are missing.
Those five-digit codes are the language of dental insurance and clinical record-keeping. They are known as ADA codes (Current Dental Terminology, or CDT codes), and they dictate how your procedure is billed, how your insurance company processes your claim, and ultimately, how much you pay out of pocket.
Understanding these codes is not about becoming a dental billing expert overnight. It is about gaining the confidence to ask the right questions. When you know what the codes mean, you can look at a $5,000 or $6,000 treatment plan and understand exactly what you are paying for.
This guide will walk you through the most common ADA dental codes for implants. We will break them down into simple, plain English, explain why there are multiple codes for what seems like one tooth, and give you the tools to review your estimate with clarity.
Why Understanding ADA Dental Codes Matters for You
Before we dive into the specific numbers, it is helpful to understand why these codes exist in the first place. The American Dental Association (ADA) publishes the CDT code set. These codes standardize dental procedures so that a dentist in New York and a dentist in California are using the same language to describe the same work.
For you, the patient, this standardization is a double-edged sword. On one hand, it ensures transparency. You can compare treatment plans (to a certain extent) because the codes are universal. On the other hand, dental insurance companies use these codes to determine what they consider “covered” and what they consider “not covered.”
Here is the reality: dental implants are frequently classified as a “major” restorative procedure. Many insurance plans consider the implant itself (the post) as a separate entity from the crown (the tooth on top). This separation is where patients often get confused.
When you understand the codes, you can:
-
Verify that your treatment plan includes all phases of the implant process.
-
Ask your insurance provider specific questions about coverage for each code.
-
Avoid unexpected bills when moving from one phase of treatment to the next.
Let’s look at the specific codes you are likely to see.
The Core ADA Codes for Dental Implants
A single dental implant is rarely a single procedure. In the world of CDT codes, it is a journey broken down into three to four distinct steps, each with its own code.
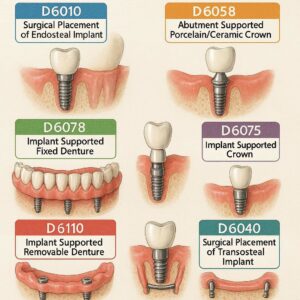
D6010: The Surgical Placement of the Implant Body
This is the foundation code. D6010 represents the surgical placement of the implant body—the titanium post that is placed into your jawbone to act as the artificial root.
If you see this code on your treatment plan, it covers the surgical time, the implant component itself, and the expertise required to place it into the bone.
Important Note: This code is often the one that insurance companies scrutinize the most. Many older plans have a “missing tooth clause,” meaning they will not pay for an implant to replace a tooth that was missing before the insurance policy started. Others may cover this code at 50% after you meet your deductible.
D6056: The Abutment
After the implant is placed and has healed (osseointegrated—a fancy word meaning the bone has grown around the post), the dentist needs to attach a connector piece. This is called the abutment. The code for a prefabricated abutment is D6056.
Think of the implant as a wall anchor. The abutment is the screw that sticks out of the wall that you actually hang the picture on.
Sometimes, you will see a code for a custom abutment (D6057). A custom abutment is milled specifically for your gum tissue shape to ensure the final crown fits perfectly and looks natural. Custom abutments are generally more expensive than prefabricated ones, but they often yield a better aesthetic result.
D6058 through D6065: The Prosthesis (The Crown)
This is the part you see and use to chew. The codes for the crown vary depending on what material is used and how it attaches to the abutment.
-
D6058: Abutment supported porcelain/ceramic crown. This is the most common code for a single implant crown made of high-strength ceramic.
-
D6062: Abutment supported cast metal crown (less common for front teeth, sometimes used for back molars).
-
D6065: Implant supported porcelain/ceramic crown (this code is used when the crown is screwed directly into the implant without a separate abutment, though this is less common today).
For most patients receiving a high-quality, natural-looking implant, D6058 is the code you will see paired with D6056.
D6110 and D6111: Implant Supported Dentures
If you are replacing an entire arch (full upper or lower teeth) rather than a single tooth, the codes change significantly.
-
D6110: Implant supported overdenture, maxillary (upper arch).
-
D6111: Implant supported overdenture, mandibular (lower arch).
These codes are comprehensive. They cover the bar, the attachments, and the denture that snaps onto the implants. These are complex cases and the costs associated with these codes are substantially higher than single-tooth codes.
A Side-by-Side Comparison: Single Tooth Implant vs. Full Arch
To help visualize how these codes stack up, here is a typical breakdown for two common scenarios.
| Treatment Phase | Single Tooth Implant (Code) | Full Arch Lower (Code) |
|---|---|---|
| Surgery | D6010 (Implant placement) | D6010 x 4-6 (Multiple implants) |
| Abutment | D6056 (Prefabricated abutment) | D6057 (Custom abutment/bar) |
| Bone Grafting (if needed) | D6011 (or D4263/D4264) | D4263/D4264 (Bone graft) |
| Final Tooth | D6058 (Porcelain crown) | D6111 (Implant overdenture) |
| Extraction (if needed) | D7140 (Extraction) | D7140 (Extraction) |
As you can see, a single tooth involves three primary codes: surgery, abutment, crown. A full arch involves multiple iterations of the surgery code plus a different final prosthesis code.
Additional Codes You Will Likely See (The “Supporting Cast”)
Implants rarely happen in a perfect, sterile environment. Often, there are prerequisites or complications that require additional codes. These ancillary codes can significantly impact the total cost.
Bone Grafting (D4263, D4264, D6011)
For an implant to be successful, you need enough healthy bone. If you have lost bone due to gum disease or the original tooth being missing for too long, you may need a bone graft.
-
D4263: Bone replacement graft, retained natural tooth (often used for sockets).
-
D4264: Bone replacement graft, each additional site (if multiple areas are grafted).
-
D6011: This is a specific code for “bone grafting at time of implant placement.” If your dentist places a graft and the implant in the same visit, they often use this code instead of the general grafting codes.
Sinus Lift (D7950, D7951, D7952)
If you are missing upper back teeth (molars), the maxillary sinus cavity sits just above the roots. When those teeth are lost, the sinus can expand downward, leaving no bone for an implant. A sinus lift involves adding bone to that area.
-
D7950: Sinus augmentation via a lateral window approach (a more invasive, traditional sinus lift).
-
D7951: Sinus augmentation via a crestal approach (a less invasive method done through the implant site).
If you see this code on your treatment plan, it explains why the cost for an upper molar implant might be higher than for a lower molar.
Extraction (D7140, D7210)
If the tooth you are replacing is still in your mouth, it must come out first.
-
D7140: Extraction, erupted tooth (a simple extraction).
-
D7210: Surgical extraction (if the tooth is broken off at the gum line or impacted).
Sometimes, a dentist will perform the extraction and place the bone graft at the same time. When this happens, you will see both codes on the same day.
CT Scan (D0367 or D0368)
Modern implant placement is often guided by 3D imaging. This is not the same as the small x-ray they take during a cleaning.
-
D0367: Cone beam CT (CBCT) scan for implant planning. This allows the dentist to see the bone in three dimensions to avoid nerves and sinuses.
The Reality of Dental Insurance and Implant Codes
This is where we need to be honest. Reading about codes is helpful, but understanding how insurance interacts with these codes is where the real value lies.
Dental insurance was designed in the 1960s and 1970s. Back then, the standard of care for a missing tooth was a bridge (code D6240, for example) or a partial denture. Implants were considered experimental.
Even today, despite implants being the gold standard of care, many insurance plans treat them as a luxury rather than a necessity.
The “Yearly Maximum” Trap
Most dental insurance plans have a yearly maximum—usually between $1,000 and $2,000. If you are getting a single implant, the total cost using the codes above (D6010, D6056, D6058) is often between $4,000 and $6,000.
If your insurance covers implants at 50% (which is generous), they would pay roughly $2,000 to $3,000. However, if your yearly maximum is only $1,500, they will stop paying once they hit that cap. You are responsible for the rest.
This is why you often see implant treatment plans broken out over two calendar years. A dentist might place the implant (D6010) in November, and place the crown (D6058) in January of the next year. This allows the patient to use two years’ worth of insurance maximums to offset the cost.
The “Downgrade” Clause
Some insurance companies will not pay the full amount for the codes associated with implants. Instead, they “downgrade” the procedure to the cheapest alternative.
For example, if you are missing tooth #19 (a molar), your insurance might say: “We don’t cover D6010 (implant), but we do cover D6240 (porcelain fused to metal bridge) for that missing tooth.” They will pay the cost equivalent of the bridge toward your implant treatment.
This helps reduce your bill, but it usually leaves a significant balance remaining.
How to Read a Treatment Plan: A Practical Walkthrough
Let us imagine you walk into a dental office. You are missing tooth #14 (upper left first molar). The dentist recommends an implant. You receive a treatment plan that looks like this:
| Code | Description | Fee | Insurance Est. | Patient Est. |
|---|---|---|---|---|
| D7140 | Extraction | $250 | $150 | $100 |
| D4263 | Bone Graft | $600 | $0 | $600 |
| D6010 | Implant Placement | $1,800 | $900 | $900 |
| D6056 | Abutment | $600 | $300 | $300 |
| D6058 | Crown | $1,800 | $900 | $900 |
| Total | $5,050 | $2,250 | $2,800 |
Here is what is happening in this plan:
-
Extraction (D7140): The old tooth is removed. Insurance usually covers this, though often at 80%.
-
Bone Graft (D4263): The patient needed a graft. Many insurance plans classify grafting as “surgical” or “minor bone grafting” and either do not cover it, or cover it at a lower percentage.
-
Implant (D6010): The core procedure. In this scenario, insurance is covering 50% (common for major services).
-
Abutment (D6056) & Crown (D6058): Also covered at 50%.
The patient is responsible for the remaining $2,800. If the yearly maximum for this plan is $1,500, the “Insurance Est.” column would be capped at $1,500, making the patient portion $3,550.
Common Questions Patients Ask About Implant Codes
Navigating these numbers can raise a lot of questions. Here are some of the most frequent concerns we hear from patients reviewing their codes.
Why is there a separate code for the abutment and the crown? Why can’t it just be one?
This is a very common point of confusion. The reason is rooted in the timeline of the procedure. The abutment (D6056) is often placed during a minor surgical visit after the implant has healed. The crown (D6058) is placed weeks later after the gums have healed around the abutment.
Because these visits occur at different times and involve different materials (titanium abutment vs. ceramic crown), the ADA requires separate codes. It also allows insurance to process them as they occur. If your plan year resets between the abutment placement and the crown seating, it can affect your benefits.
What if my dentist uses a different code than the one listed here?
There are over 700 CDT codes. While the codes listed above are the most common for implants, there are variants. For example, you might see D6066 (Implant supported crown, with a metal/ceramic combination) or D6070 (Re-cement or repair of implant crown).
If you see a code that does not match the ones listed here, do not panic. Simply ask your treatment coordinator: “I see code XYZ on my plan. Can you explain what that code covers and why it is being used instead of the more common D6010 for the implant?” A good office will be happy to explain the nuance.
Will insurance cover the “final” code (the crown) if I switch dentists?
This is a tricky scenario. If your surgeon places the implant (D6010) and then you move or decide to go to your general dentist for the crown (D6058), you need to ensure the insurance codes align.
Sometimes, insurance companies want to see that the same provider did the entire case. If you split the treatment, make sure both providers are in-network (if that matters to you) and that the referring dentist sends the necessary notes (like the implant log) to the restorative dentist so they can bill the crown correctly.
Strategies to Maximize Your Insurance Benefits
Understanding the codes gives you a strategic advantage. Here are a few practical strategies to make the most of your dental benefits when facing implant treatment.
1. Ask for a “Pre-Treatment Estimate”
Before any work is done, ask your dentist to send the codes to your insurance company for a pre-treatment estimate (also called a predetermination). This is not a guarantee of payment, but it is a good-faith estimate of what the insurance company intends to pay for each specific code. It costs you nothing and prevents surprise bills.
2. Phase Your Treatment
As mentioned earlier, look at the calendar. If you need an extraction, graft, and implant placement, can you do that in October? If you wait until January to do the abutment and crown, you reset your deductible and yearly maximum. It is a legitimate way to save money, and most dentists are accustomed to planning treatment this way.
3. Check for Medical vs. Dental Coverage
This is a high-level strategy. Some implant procedures, particularly those involving bone grafting (D4263) or sinus lifts (D7950), can sometimes be billed to medical insurance if there is a clear pathology (like a cyst, tumor, or congenital defect).
While this does not apply to standard tooth replacement, if your implant is necessary due to trauma or a medical condition, ask your dentist’s billing coordinator if they have successfully billed medical insurance for similar cases. Medical insurance often has higher yearly maximums than dental insurance.
The Value Beyond the Codes
While this article focuses heavily on the financial and procedural codes, it is worth taking a moment to reflect on what these codes represent.
When you pay for D6010, you are paying for the precision of surgical placement—ensuring the post avoids nerves and integrates with bone.
When you pay for D6056 and D6058, you are paying for the artistry of the restorative dentist—matching the color, shape, and contour of the crown to your natural teeth so that it blends seamlessly.
Dental implants are an investment in your long-term health. Unlike a bridge, which requires shaving down healthy adjacent teeth, an implant stands alone. It preserves bone density. It allows you to chew with the same force as a natural tooth.
Understanding the codes does not make the investment smaller, but it removes the mystery. It allows you to be an active participant in your healthcare decisions rather than a passive recipient of a bill.
How Technology is Changing Implant Billing
The codes we have discussed are the standard today, but the landscape is shifting. With the rise of same-day implants and guided surgery, the way these procedures are billed is evolving.
Some practices are now using D6012 (Surgical placement of an implant, including placement of a prefabricated abutment and crown). This is a “bundled” code that combines the implant, abutment, and crown into one code. This is often used in “teeth-in-a-day” procedures where the patient walks out with a fixed tooth on the same day as the surgery.
However, this code is not yet accepted by all insurance companies. Many still prefer to see the traditional breakdown (D6010, D6056, D6058) because it allows them to apply different coverage percentages to the surgical portion versus the restorative portion.
If your dentist offers a bundled service, ask to see the itemized codes. You want to ensure that if there is a complication with the implant later (a rare occurrence), the warranty or guarantee covers all the components, not just the crown.
Avoiding Common Billing Mistakes
Even with the best intentions, mistakes happen. Being an informed patient helps you catch errors before they become costly.
-
Duplicate Codes: Ensure that if you are having four implants placed, you are charged for D6010 four times, not once. Some billing software can accidentally lump them together incorrectly.
-
Wrong Tooth Number: Codes are usually accompanied by a tooth number (e.g., #14, #3, #19). Double-check that the tooth number on the treatment plan matches the tooth that is actually being treated. This is a common clerical error.
-
Unbundling: This is a term used when a dentist bills for separate components that should be included in a single code. For example, if a dentist bills for “surgical guide” as a separate code (often D6190) but the implant placement code (D6010) already includes the cost of the guide, this is considered unbundling. Always ask: “Is this code separate, or is it usually included in the main procedure?”
A Note on “Out-of-Network” Providers
If you choose a dentist who is out-of-network with your insurance, the codes still apply. However, the “allowed amount” changes.
In-network dentists have a contract with the insurance company that caps the fees for each code. Out-of-network dentists do not have that cap. They can charge their full fee.
If you have an out-of-network dentist, your insurance company will still process the claim using the codes. They will calculate what they would have paid an in-network dentist for that code (the UCR, or Usual, Customary, and Reasonable fee) and pay you or the dentist that amount. You are responsible for the difference between the dentist’s fee and the insurance payment.
This is not necessarily a bad thing—sometimes the quality of care or the technology used by an out-of-network specialist is worth the extra cost. But you should be aware of it upfront.
Conclusion
Navigating the world of ADA dental codes for implants does not require a degree in medical billing. It requires curiosity and a willingness to ask questions. By familiarizing yourself with codes like D6010 (the implant), D6056 (the abutment), and D6058 (the crown), you transform a confusing estimate into a clear roadmap of your treatment.
Remember, these codes are tools for communication. Use them to facilitate conversations with your dentist and your insurance provider. A clear understanding of what you are paying for—and why—will give you peace of mind throughout the implant process. Ultimately, this knowledge empowers you to make the best decision for your oral health, ensuring that your investment is sound and your smile is secure for years to come.
Frequently Asked Questions (FAQ)
1. What is the ADA code for a single tooth implant?
There is no single code for a full implant. The process uses a combination of codes. The main codes you will see are D6010 (surgical placement of the implant body), D6056 (abutment), and D6058 (implant supported crown).
2. Does dental insurance cover D6010?
It depends on your specific plan. Many plans cover implants as a “major” service, typically at 50% after the deductible. However, some plans specifically exclude implants (D6010) altogether, or have a “missing tooth clause” that denies coverage if the tooth was missing before the policy started.
3. Why was I charged for a bone graft code (D4263) if I didn’t know I needed it?
Bone grafting is often discovered during the planning phase. If you have been missing a tooth for a long time or had an infection, bone loss is common. A CBCT scan (D0367) often reveals the need for a graft. It is a necessary step to ensure the implant has enough bone to fuse to.
4. What is the difference between D6056 and D6057?
D6056 is a prefabricated abutment, which is a stock piece made by the implant manufacturer. D6057 is a custom abutment, which is milled specifically for your gum contour to provide a more aesthetic, custom fit. Custom abutments usually cost more.
5. Can I get an implant if my insurance doesn’t cover D6010?
Yes. Many patients pay for implants out-of-pocket or use financing options like CareCredit. Even if insurance does not cover the implant post (D6010), they may still cover the crown (D6058) as a “bridge alternative” or cover the extraction (D7140). Discuss a phased payment plan with your dental office.