D2949 Dental Code: Restorative Indirect Pulp Therapy
- On
- InDENTAL CODE
If you have spent any time around dental billing or treatment planning lately, you have likely encountered a code that did not exist a few years ago: D2949. It sounds technical. It looks official. But what does it actually mean for you—whether you are the person diagnosing, the person paying, or the person sitting in the chair?
This guide is designed to answer that question clearly, without jargon for the sake of jargon. We will walk through what this code covers, when it should be used, how it differs from other procedures, and—perhaps most importantly—what it means for your wallet and your oral health.
Consider this your trusted, no-hype manual. Let us begin.

Table of Contents
ToggleWhat Is the D2949 Dental Code? A Straightforward Definition
Let us start with the basics. The D2949 dental code officially describes a procedure called “restorative indirect pulp therapy.”
If you break that down, it sounds more complicated than it actually is.
-
Restorative: This means the tooth is being repaired or restored to function.
-
Indirect: The treatment does not involve direct contact with the dental pulp (the living tissue deep inside the tooth).
-
Pulp therapy: The goal is to protect and preserve the pulp so it remains healthy.
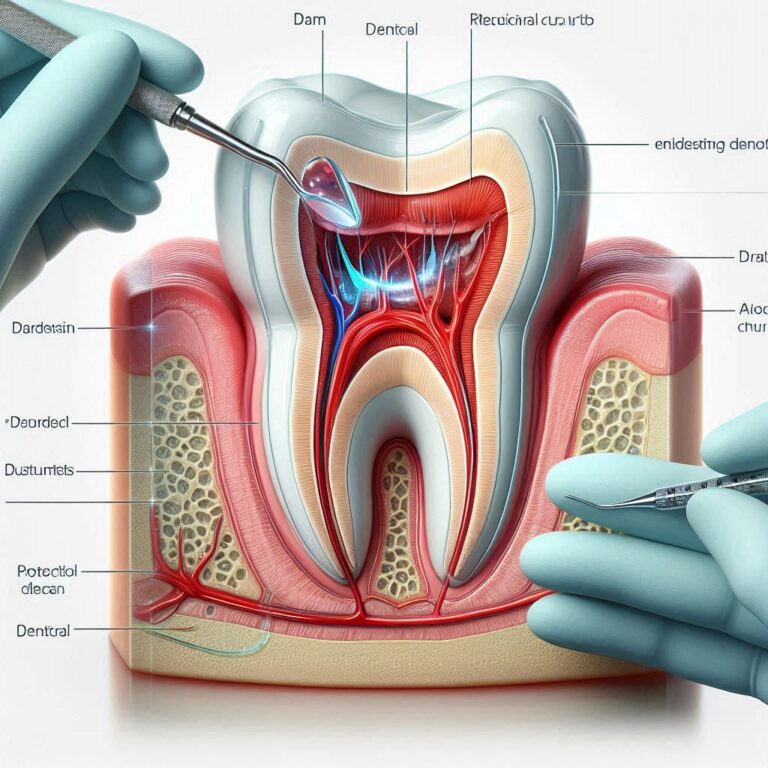
In plain language: D2949 is used when a dentist removes decay from a tooth but intentionally leaves a thin layer of softened dentin near the pulp to avoid exposing the nerve. They then place a medicated or protective liner and restore the tooth, usually with a permanent filling.
The entire point is prevention. Instead of risking an exposed nerve—which would require more invasive treatment like a root canal—the dentist stops just short, seals the tooth, and allows the pulp to recover on its own.
“Indirect pulp therapy is one of the most conservative approaches we have. It respects the tooth’s natural healing ability while removing active disease.” — Dr. Elena Marques, DDS, restorative dentistry educator
Why Was D2949 Introduced? The Gap It Fills
You might wonder: was this not already covered by other codes? The short answer is no—not accurately.
Previously, dentists had limited options when documenting this specific procedure. Many used:
-
D3110 – Pulp cap (direct or indirect) – historically vague and inconsistently applied.
-
D2140 through D2161 – Amalgam or resin fillings – which describe the restoration, not the pulp-protection step.
-
D2940 – Protective restoration – often a sedative filling but not necessarily definitive.
The result was inconsistent record-keeping and, at times, confusion with insurance payers. D2949 was introduced by the American Dental Association (ADA) in 2021 to bring clarity. It acknowledges that indirect pulp therapy is a distinct clinical skill requiring time, expertise, and specific materials—not just a routine filling.
This code validates that the dentist performed an intentional therapeutic step to save the tooth from more extensive treatment.
D2949 vs. Other Pulp Therapy Codes: A Side-by-Side Comparison
One of the most common points of confusion is how D2949 differs from similar-sounding codes. Let us clear that up.
| Code | Procedure | Key Difference |
|---|---|---|
| D2949 | Restorative indirect pulp therapy | Decay left near pulp; tooth restored same visit. Goal: avoid pulp exposure. |
| D3110 | Pulp cap – direct or indirect | Vague. Often used for small exposures or shallow liners. Being phased out in favor of more precise codes. |
| D3120 | Pulp cap – direct (final restoration) | Used when pulp is visibly exposed and capped. Not indirect. |
| D3220 | Therapeutic pulpotomy | Partial removal of pulp tissue. Typically for primary teeth or irreversible damage. |
| D3221 | Pulpal debridement | Temporary procedure for pain relief. Not definitive. |
| D2940 | Protective restoration | Sedative dressing. Often temporary. Not always followed by final restoration. |
Important note: D2949 assumes the final restoration is placed during the same appointment, or at least that the definitive restorative plan is underway. It is not a temporary patch.
When Is D2949 Used? Realistic Clinical Scenarios
Not every cavity qualifies for D2949. This procedure is appropriate only under specific conditions.
Suitable Situations
-
Deep carious lesion approaching the pulp, but no signs of irreversible pulpitis.
-
Asymptomatic tooth or reversible pulpitis only.
-
Clinically healthy pulp response (no spontaneous pain, no lingering pain to cold).
-
Ability to isolate the tooth (rubber dam preferred).
-
Patient is not allergic to materials used.
Unsuitable Situations
-
Pulp exposure has already occurred.
-
Tooth is non-vital or necrotic.
-
Swelling, fistula, or radiographic sign of apical pathology.
-
Patient reports severe, lingering, or spontaneous pain.
-
Tooth cannot be adequately restored after procedure.
“If the pulp is already infected or dying, indirect pulp therapy will not save it. You are just putting a nice filling over a failing tooth.” — Dr. Robert Chin, endodontist
Step by Step: What Happens During a D2949 Procedure?
If you are a patient scheduled for this treatment, here is what a typical appointment looks like. If you are a professional, consider this a communication tool to share with your patients.
1. Diagnosis and treatment planning
Your dentist examines the tooth, reviews X-rays, and tests pulp vitality. They explain that the decay runs deep but they believe the nerve can be saved without direct exposure.
2. Local anesthesia
The tooth and surrounding area are numbed. Comfort is essential for precise work.
3. Isolation
A rubber dam is placed. This keeps the tooth dry, clean, and free of saliva. It also prevents debris from entering the throat.
4. Decay removal
The dentist removes most of the decay using hand instruments or a slow-speed handpiece. They stop when removing more would risk exposing the pulp. A small amount of softened dentin may remain at the deepest part.
5. Medicament placement
A biocompatible material is placed over the remaining affected dentin. Common options include:
-
Calcium hydroxide
-
Mineral trioxide aggregate (MTA)
-
Resin-modified glass ionomer
This layer encourages healing, remineralization, and forms a barrier against bacteria.
6. Base or liner
A protective base may be placed over the medicament to support the final restoration.
7. Final restoration
The tooth is restored, typically with a permanent material such as composite resin, amalgam, or sometimes stainless steel crown (especially in children). The bite is checked and adjusted.
8. Post-operative instructions
You may experience mild cold sensitivity for a few days. Normal oral hygiene is encouraged. A follow-up is scheduled to monitor the tooth.
Success Rates: Is Indirect Pulp Therapy Reliable?
Let us be honest. No dental treatment works 100% of the time. But the evidence for indirect pulp therapy is surprisingly strong.
Studies consistently report success rates between 80% and 95% over a 2-to-5-year period when appropriate case selection is used. The key variable is not the material—it is the pre-operative pulp status.
If the pulp is healthy or reversibly inflamed, the prognosis is excellent. If the pulp is already degenerating, the procedure will fail.
Factors that improve success:
-
No history of spontaneous pain.
-
Rubber dam isolation.
-
Proper hermetic seal with the final restoration.
-
Patient maintains good oral hygiene.
Factors that lower success:
-
Contamination during procedure.
-
Leaking or defective restoration.
-
Delayed final restoration.
-
Uncontrolled caries in other areas.
Insurance Coverage and Reimbursement: What Patients Need to Know
This is the part that often frustrates both dentists and patients. D2949 is a relatively new code, and insurance coverage varies widely.
What to Expect
-
Medical necessity: The procedure must be justified with radiographs and pulp testing results. A simple note saying “deep decay” is often insufficient.
-
Frequency limitations: Most plans limit D2949 to once per tooth per lifetime, or once every 2–3 years.
-
Downgrading: Some carriers automatically downcode D2949 to D2940 or a routine filling code, reimbursing at a lower rate.
-
Patient responsibility: If the plan does not recognize D2949, the patient may be responsible for the difference between the allowed amount and the provider’s fee.
Always verify benefits before treatment. Ask your dentist’s office to send a pre-determination of benefits to your insurance company. This is not a guarantee of payment, but it reduces surprises.
“Insurance companies are always playing catch-up with clinical codes. We have to advocate for our patients and document thoroughly.” — Sarah Kline, RDH, practice administrator
D2949 in Pediatric Dentistry: A Special Focus
While D2949 applies to any age, it is particularly relevant in children. Primary teeth have thinner enamel and larger pulp chambers, making deep decay a common challenge.
In pediatric patients, indirect pulp therapy offers several advantages:
-
Avoids pulp exposure and the need for pulpotomy or pulpectomy.
-
Maintains tooth structure.
-
Often completed in one visit.
-
Preserves the tooth until natural exfoliation.
Many pediatric dentists consider D2949 the standard of care for deep caries in asymptomatic primary molars. It is less invasive than pulpotomy and supports the tooth’s natural healing.
Important distinction: In primary teeth, the final restoration may be a stainless steel crown. This is still reportable with D2949 plus the crown code, provided the pulp therapy was performed.
Documentation and Coding Tips for Dental Professionals
Accurate documentation is essential—not only for reimbursement but for legal and clinical records. If you are a dentist or a billing specialist, here is what payers expect to see.
Essential elements in the patient record:
-
Pulp vitality test results (cold, EPT, or both).
-
Radiographic evidence of deep caries approximating the pulp.
-
Description of decay removal technique.
-
Type and brand of medicament placed.
-
Material used for the final restoration.
-
Post-operative instructions.
-
Follow-up plan.
Common denial reasons and how to avoid them:
-
“Procedure not medically necessary.” – Include pulp testing and a narrative explaining why indirect therapy was chosen over root canal or extraction.
-
“Already included in restoration code.” – Clarify that D2949 is a distinct therapeutic procedure, not part of the filling. Use modifier -25 if billing with an exam or other procedure on the same day.
-
“Frequency limitation exceeded.” – Verify prior claims on the same tooth before submitting.
Common Myths About D2949
Let us clear up a few persistent misunderstandings.
Myth 1: D2949 is just an expensive filling.
Reality: It includes a therapeutic step not present in a standard restoration. The medicament, technique, and clinical judgment required are distinct.
Myth 2: It is only for baby teeth.
Reality: It is used in both primary and permanent teeth. In adults, it can delay or prevent root canal therapy.
Myth 3: Leaving decay is bad dentistry.
Reality: Only affected (remineralizable) dentin is left. Infected, necrotic dentin is always removed. This is a biologically sound, evidence-based approach.
Myth 4: Insurance always covers it.
Reality: Coverage is inconsistent. Many plans still treat it as experimental, despite strong evidence and ADA recognition.
The Future of D2949 and Minimally Invasive Dentistry
D2949 is not an isolated code. It is part of a larger shift in dentistry: moving away from “extension for prevention” and toward minimally invasive, biologically respectful care.
As research continues to support the pulp’s capacity for healing, we can expect:
-
Broader insurance acceptance.
-
Increased adoption in dental schools.
-
Refinement of materials specifically designed for indirect pulp therapy.
-
Potential new codes for biologically based treatments.
For now, D2949 represents a middle ground—a way to buy time, preserve tissue, and make treatment less aggressive without compromising outcomes.
Summary Table: Key Facts About D2949
| Aspect | Detail |
|---|---|
| Full description | Restorative indirect pulp therapy |
| Year introduced | 2021 (ADA Code Maintenance Committee) |
| Goal | Avoid pulp exposure; maintain pulp vitality |
| Tooth types | Primary and permanent |
| Typical fee range | $50–$150 (geographic and provider dependent) |
| Success rate | 80–95% with proper case selection |
| Common payers | Delta Dental, Cigna, MetLife, BCBS (varies by plan) |
| Main alternative | Direct pulp cap (D3110), pulpotomy (D3220), root canal (D3310) |
Frequently Asked Questions (FAQ)
1. Is D2949 considered a major or basic service?
It varies by carrier. Some classify it as basic restorative; others consider it an endodontic procedure. Check your specific plan.
2. Can D2949 and D2391 (composite filling) be billed together?
Yes. D2949 describes the pulp therapy; the restoration code describes the filling. Both are separately reportable when performed.
3. Does D2949 require a rubber dam?
While not an absolute requirement, rubber dam isolation is strongly recommended and considered best practice for predictable success.
4. How long does a D2949 procedure take?
Typically 30 to 60 minutes, depending on tooth location, extent of decay, and restorative material.
5. Will I need a follow-up appointment?
Yes. Most dentists recommend clinical and radiographic evaluation at 6 months and annually thereafter.
6. Can the same tooth receive D2949 more than once?
Technically yes, if new decay develops and the pulp remains vital. However, insurance may not cover a second application.
7. Does D2949 guarantee I won’t need a root canal?
No. It significantly reduces the risk, but some teeth will eventually require endodontic treatment despite best efforts.
Additional Resource
For clinicians seeking a deeper dive into the evidence base and technique protocols, the following resource is invaluable:
➡️ American Academy of Pediatric Dentistry: Pulp Therapy for Primary and Immature Permanent Teeth
This guideline includes detailed comparisons of indirect pulp therapy vs. pulpotomy, material recommendations, and long-term outcome data.
Conclusion
The D2949 dental code fills a long-standing gap in how we document and value conservative pulp therapy. It acknowledges that preserving pulp health requires skill, judgment, and specific materials—distinct from a routine filling. For patients, it offers a chance to avoid more invasive treatment. For dental teams, it provides a standardized way to communicate what was done and why. As minimally invasive dentistry continues to evolve, D2949 is likely to become not just an option, but a benchmark of modern care.

dentalecostsmile
Newsletter Updates
Enter your email address below and subscribe to our newsletter