Zygomatic Dental Implants
If you have been told that your upper jaw bone is too thin or too soft for traditional dental implants, you already know how frustrating that news can be. Many people walk away from a dentist’s office feeling hopeless. They hear words like “severe bone loss” or “sinus cavities” and think their only option is a removable denture that slips, clicks, or causes sore spots.
But there is another path.
Zygomatic dental implants have changed the game for people with significant bone loss in the upper jaw. Instead of relying on the maxilla (the upper jawbone), these longer implants anchor into the zygomatic bone—better known as your cheekbone. This is one of the strongest bones in your skull.
In this guide, we will walk you through everything you need to know. No fluff. No fake claims. Just honest, practical information to help you make an informed decision.
What Exactly Are Zygomatic Dental Implants?
Let’s start with the basics.
Traditional dental implants are small titanium screws placed directly into your jawbone. They need enough bone height and width to fuse properly. For the upper jaw, that means you need at least 8 to 10 millimeters of bone beneath your sinuses.
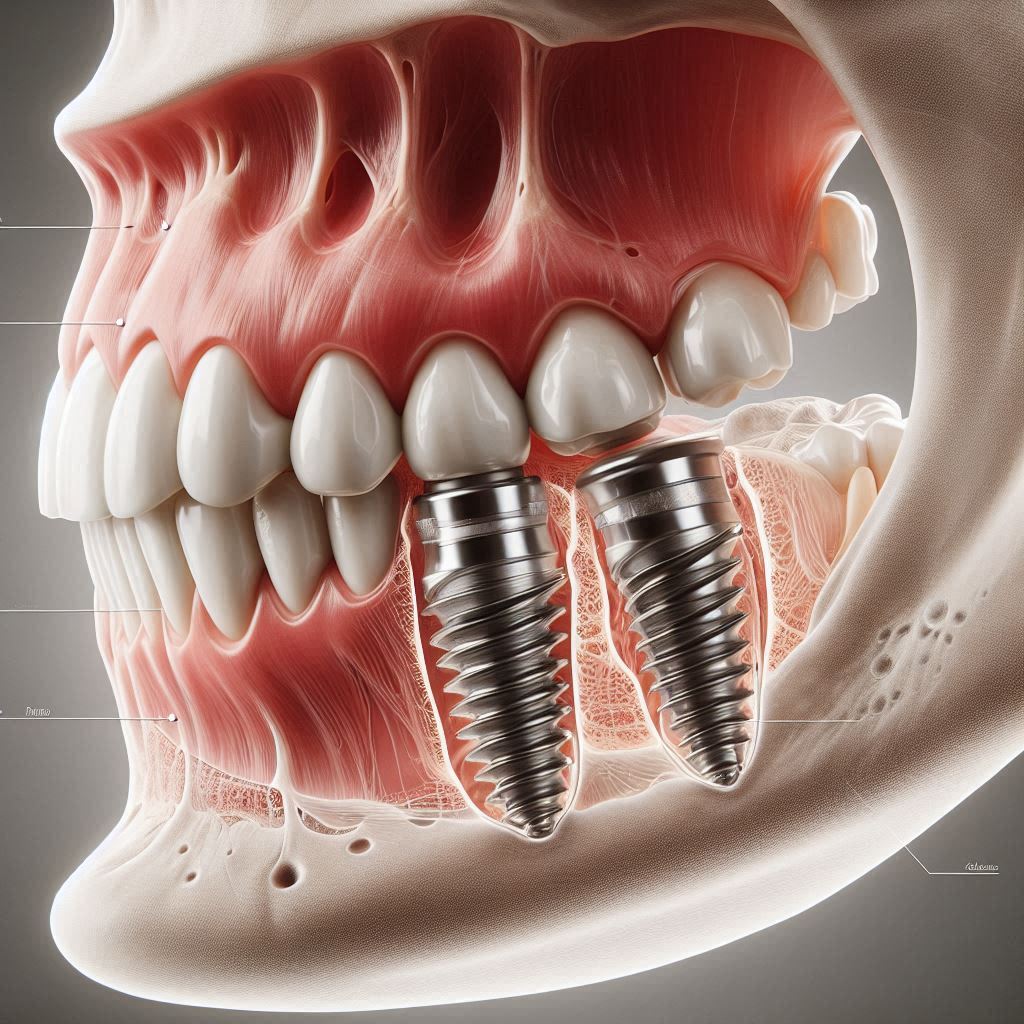
Zygomatic implants are much longer—typically between 30 and 52 millimeters. Instead of standing straight up inside the jaw, they take a longer route. The implant starts where a normal tooth root would go but then angles backward and upward. It passes through the maxillary sinus (the empty space behind your cheek) and finally anchors into the zygomatic bone.
That cheekbone connection is the secret sauce. The zygomatic bone is dense and stable, even in patients who have lost almost all of their upper jawbone due to gum disease, injury, or long-term denture wear.
Important note: Zygomatic implants are not for everyone. They are a specialized solution for severe upper jaw atrophy. Your dentist or oral surgeon will perform detailed imaging (like a CBCT scan) to see if your anatomy fits the requirements.
A Quick Comparison
| Feature | Traditional Implants | Zygomatic Implants |
|---|---|---|
| Typical length | 8–16 mm | 30–52 mm |
| Anchor point | Upper jawbone (maxilla) | Cheekbone (zygomatic bone) |
| Bone graft needed? | Often yes, if bone is lacking | No |
| Sinus involvement | Usually avoid the sinus | Passes through the sinus |
| Number of implants for full arch | 6–8 traditional implants | 4 zygomatic implants |
| Treatment time (to final teeth) | 6–12 months | Often 1–3 months |
Who Really Needs Zygomatic Implants?
This is not a first-line treatment. No ethical dentist would recommend zygomatic implants if traditional implants or bone grafting could work just as well.
So, who is the ideal candidate?
Severe Maxillary Bone Atrophy
This is the number one reason. When the upper jawbone has resorbed (melted away) to the point where it is 4 millimeters or thinner in the central areas, traditional implants become risky. Placing a standard implant in such thin bone would likely pierce through to the nose or sinus cavity.
Five millimeters or less of bone height is generally the threshold where zygomatic implants become a serious consideration.
Failed Sinus Lifts or Bone Grafts
Some patients have already tried bone grafting. They underwent a sinus lift procedure, waited months for healing, and then were told the graft did not take. Maybe the bone resorbed again, or an infection ruined the graft.
Zygomatic implants bypass this problem entirely. They do not rely on grafted bone.
Long-Time Denture Wearers
When you wear a removable upper denture for 15, 20, or 30 years, the constant pressure accelerates bone loss. The denture rests on your gums, but the underlying bone gradually disappears. Many long-term denture wearers end up with a jawbone as thin as an eggshell. For them, zygomatic implants offer a way to finally have fixed teeth.
Tumor or Trauma Survivors
People who have had a maxillectomy (surgical removal of part of the upper jaw) due to cancer or severe facial trauma often lack the bone needed for normal implants. Zygomatic implants can bridge those defects and provide stable anchors for a dental prosthesis.
Honest warning: Zygomatic implant surgery is more complex than traditional implant placement. You need a surgeon who has performed dozens, ideally hundreds, of these procedures. Do not let a general dentist convince you to be their first zygomatic case.
How Do Zygomatic Implants Differ From Standard Implants?
Let’s put them side by side in a different way so you can truly see the differences in real-world terms.
The Path They Take
A standard implant enters at the top of the gum ridge and travels straight down into the jawbone. Straight path. Short distance.
A zygomatic implant enters near the back of your upper gum (where your first or second molar used to be) and then travels diagonally upward and backward. It passes right through the sinus cavity—which is normally empty air—and comes to rest inside your cheekbone. The tip of the implant actually sits near your eye socket, but safely so.
That diagonal path gives it incredible stability. Once the bone grows around it (a process called osseointegration), that implant is extremely strong.
The Number of Implants Needed
For a full upper arch of teeth (all 14 teeth in your upper jaw), traditional implant protocols typically require 6 to 8 implants spread across the jawbone.
With zygomatic implants, many patients receive only 4 total implants: two zygomatic implants in the back (one on each side) plus two traditional implants in the front of the jaw (where bone might still be decent).
That combination is often called the “quad zygoma” or “zygoma with anterior regular implants.” Some severe cases use four zygomatic implants alone, with no traditional implants at all.
The Loading Protocol
Traditional implants almost always require a healing period of 3 to 6 months before you can attach permanent teeth. During that time, you wear a provisional denture.
Zygomatic implants are often “immediately loaded.” This means you walk out of the surgery with a fixed temporary bridge attached to the implants the same day. Of course, you will need soft foods and careful cleaning, but you have teeth that do not come out.
That immediate result is a huge quality-of-life advantage.
The Step-by-Step Procedure: What Actually Happens?
Let’s walk through the entire journey—from your first consultation to eating an apple again. We will be honest about the good and the not-so-fun parts.
Step 1: Comprehensive Evaluation (1–2 hours)
Your journey begins with imaging. A standard X-ray is not enough. You need a CBCT scan (cone beam computed tomography). This gives your surgeon a 3D map of your skull, including:
- The exact thickness of your remaining jawbone
- The position and size of your sinuses
- The shape and density of your zygomatic bones
- The location of nerves and blood vessels
Your surgeon will also review your medical history. Conditions like uncontrolled diabetes, heavy smoking (more than a pack a day), or certain autoimmune diseases may increase risks. You must be healthy enough for a longer surgery under general anesthesia or IV sedation.
Step 2: Virtual Surgical Planning (1–2 weeks before surgery)
Using the CBCT data, your surgeon plans the exact angle, length, and entry point for each zygomatic implant. Many surgeons use specialized software to create a surgical guide. This guide fits over your gums and ensures the drill follows the perfect path.
Some practices also create a temporary bridge in advance. That way, it is ready to snap onto the implants immediately after placement.
Step 3: Surgery Day (2–4 hours)
You will be fully numb and sedated. Some surgeons prefer general anesthesia; others use deep IV sedation. You will not feel or remember the procedure.
Here is what happens inside your mouth:
- Incisions: Your surgeon makes small cuts in your gum tissue to expose the bone where each implant will go.
- Drilling: Using the surgical guide, the surgeon drills a precise channel through your jaw, through the sinus, and up into the cheekbone. This requires great skill—the angle must be perfect to avoid the eye socket or important nerves.
- Implant placement: The titanium implant is carefully screwed into place. The head of the implant (the part that will hold your tooth) sits just above your gum line.
- Repeat: The same process happens for the other zygomatic implants (usually 2 to 4 total).
- Abutment attachment: Small connector pieces (abutments) are screwed into the implants.
- Temporary bridge delivery: Your pre-made temporary bridge clicks or screws onto the abutments. At that moment, you have a full set of upper teeth again.
Realistic expectation: You will have swelling, bruising, and soreness afterward. The cheekbone area can feel tender. Plan to take at least 3–5 days off work. Some patients need a full week.
Step 4: Healing Phase (2–6 months)
Even though you have a temporary bridge right away, your body still needs time to heal. The implants must fuse with your cheekbone and any remaining jawbone. This process is called osseointegration.
During this time:
- You will eat a soft diet. No crunchy bread, steak, nuts, or raw carrots.
- You will use special rinses and a very soft toothbrush or water flosser.
- You will return for periodic checks so your surgeon can monitor healing.
The temporary bridge is usually made of acrylic or a hybrid material. It looks fine, but it is not your final set of teeth. It can chip or stain, so treat it gently.
Step 5: Final Bridge Delivery (1 appointment, about 2–3 hours)
Once your implants are fully healed and integrated (usually 4 to 6 months after surgery), your surgeon or restorative dentist will replace the temporary bridge with your permanent one.
The permanent bridge is typically made of:
- Zirconia: Extremely strong, looks very natural, but costs more.
- Acrylic with a titanium frame: Lighter and less expensive, but may need replacement after 5–10 years.
Your dentist will check your bite to ensure your top and bottom teeth meet comfortably. They will also give you detailed cleaning instructions.
Benefits of Choosing Zygomatic Implants
Why would someone choose this route over a traditional denture or bone grafting?
No Bone Grafting. Period.
This is the biggest benefit for many people. Bone grafting:
- Adds 4 to 12 months to your treatment time
- Requires a separate surgery (often more painful than implants)
- Can fail or become infected
- Costs thousands of extra dollars
Zygomatic implants skip all of that.
Fixed Teeth in One Day (Usually)
If you have been wearing a denture that moves when you laugh, sneeze, or eat, the idea of fixed teeth is life-changing. Most zygomatic patients leave the surgery center with a fixed temporary bridge. It does not come out. You do not need adhesive or paste.
You sleep in it. You eat (soft foods) with it. You smile with confidence because it will not flip up or fall out.
High Success Rates
When placed by experienced surgeons, zygomatic implants have reported success rates of 95% or higher at 5 years, and over 90% at 10 years. These numbers are very similar to traditional dental implants.
Important note: Success depends heavily on the surgeon’s skill and your commitment to oral hygiene. Smoking dramatically lowers success rates for zygomatic implants.
Preserves What Little Bone You Have
Because zygomatic implants do not rely on your jawbone for primary stability, you do not need to remove or reshape your remaining bone. In fact, the stimulation from the implants may help preserve the jawbone you still have.
Improved Quality of Life
Studies show that people with zygomatic implants eat a wider variety of foods, report higher self-esteem, and have less anxiety in social situations compared to denture wearers. These are real, measurable benefits.
Risks and Complications: Being Honest
No surgery is risk-free. Zygomatic implant surgery carries higher risks than placing a single traditional implant. You deserve to know what those risks are.
Sinus Issues
The implant passes directly through your maxillary sinus. For most people, this causes no long-term problem. The body simply adapts. However, some patients experience:
- Sinusitis (inflammation of the sinus lining)
- Feeling of pressure or fullness in the cheeks
- Nasal congestion on the side of the implant
These symptoms usually resolve within weeks. In rare cases, a patient needs endoscopic sinus surgery to remove inflamed tissue around the implant.
Nerve Injury
The infraorbital nerve runs near the cheekbone area. If the implant places pressure on this nerve, you might experience numbness in your upper lip, cheek, or nose. This numbness is often temporary but can be permanent in a small percentage of cases.
Orbital (Eye) Complications
This is rare but serious. If the implant is placed too far upward, it could penetrate the floor of the eye socket (orbit). Symptoms include double vision, eye pain, or restricted eye movement. An experienced surgeon using 3D planning should never let this happen.
Implant Failure
Zygomatic implants can fail to integrate, just like traditional implants. Signs include persistent pain, mobility of the implant, or infection that does not respond to antibiotics. Failed zygomatic implants are difficult to remove. In some cases, they are simply left in place and bypassed with another implant.
Prosthetic Complications
The bridge attached to your implants can chip, crack, or break. This is not a failure of the implants themselves but of the teeth on top. Acrylic bridges are more prone to fracture than zirconia. Good news: most fractures are repairable in the dental lab or chairside.
List of Potential Side Effects (Short-Term)
- Moderate to severe swelling (lasts 5–10 days)
- Bruising on the cheek or under the eye (looks worse than it feels)
- Temporary nasal congestion
- Sore throat from the breathing tube (if general anesthesia used)
- Difficulty opening your mouth wide (resolves in 1–2 weeks)
Zygomatic Implants vs. Alternatives: A Decision Guide
You have options. Let’s compare zygomatic implants to the other paths you could take.
| Option | Pros | Cons | Best For |
|---|---|---|---|
| Zygomatic Implants | No bone graft; fixed teeth in 1 day; high success | Complex surgery; higher cost; limited number of expert surgeons | Severe bone loss; failed grafts; denture intolerance |
| Traditional Implants + Bone Graft | Uses standard implant components; many dentists can do it | 6–12 months longer; two surgeries; graft can fail | Moderate bone loss where grafting is predictable |
| Removable Upper Denture | Least expensive; no surgery | Poor stability; accelerates bone loss; affects taste and speech | Patients who cannot have surgery or cannot afford implants |
| Implant-Supported Overdenture | More stable than regular denture; fewer implants needed (2–4) | Still removable; requires daily removal for cleaning | Moderate bone loss where 2–4 standard implants can be placed |
| Titanium Mesh + Bone Graft | Can rebuild large defects | Multiple surgeries; long healing; graft resorption possible | Young patients with trauma or congenital defects |
Real Talk: When to Choose Which
- If you have 8mm or more of bone height in the upper jaw → Try traditional implants first. No need for zygomatics.
- If you have 4–7mm of bone → You could consider a sinus lift plus traditional implants, but zygomatics are a reasonable alternative.
- If you have less than 4mm of bone → Zygomatic implants are likely your best fixed-teeth option.
- If you have already tried grafting and it failed → Do not repeat the same mistake. Go straight to zygomatics.
Costs: What Will You Really Pay?
Let’s talk money. This is not cheap. But understanding the numbers helps you plan.
Typical Cost Range for Zygomatic Implants (Full Upper Arch)
In the United States, expect to pay:
- Low end: $25,000 – $30,000 (usually with acrylic temporary bridge only, plus extra for final teeth)
- Average: $35,000 – $55,000 (includes permanent zirconia bridge)
- High end (premium centers): $60,000 – $90,000 (includes all imaging, sedation, surgical guides, and a high-end ceramic bridge)
Outside the US, prices can be lower:
- Mexico (specialized centers): $15,000 – $25,000
- Colombia: $12,000 – $20,000
- Spain or Turkey: $10,000 – $22,000
Important note: If a price seems too good to be true (like $7,000 for full zygomatic implants), it probably is. That likely covers only the implant parts, not surgery, anesthesia, imaging, or the final teeth. Read the fine print.
What’s Usually Included in a Fair Quote?
A reputable clinic will include:
- CBCT scan and surgical planning
- Sedation or general anesthesia fees
- All zygomatic and traditional implants (titanium)
- Surgical placement
- Same-day temporary fixed bridge
- Four to six follow-up visits
- The final permanent bridge (specify material in writing)
- One year of warranty on the implants and bridge
What Insurance Covers
Most dental insurance plans will not cover zygomatic implants. They often have a lifetime maximum of $1,000–$2,000, which barely makes a dent.
Medical insurance may cover part of the surgery if you have a medical condition that caused your bone loss (like a tumor or cleft palate). However, for ordinary bone loss from dentures or gum disease, medical insurance rarely contributes.
Financing Options
- CareCredit (medical/dental credit card with promotional financing)
- LendingClub (patient payment plans)
- Clinic in-house financing (some large implant centers offer 12–24 month plans)
- 401(k) loan (borrowing from yourself)
- Home equity line of credit (if you own a home)
Our advice: Do not let cost drive you to an inexperienced surgeon. Zygomatic implants are too complex to be a “bargain.” Pay for expertise. It is cheaper than fixing a botched case.
Finding an Experienced Surgeon
This is the most important decision you will make. A bad zygomatic implant case can leave you in chronic pain, with numb lips, and thousands of dollars in corrective bills.
What to Look For
- Board certification in oral and maxillofacial surgery (OMFS) is a must. Period.
- Case volume: Ask, “How many zygomatic implant cases have you done personally?” If the answer is less than 50, walk away.
- CBCT on site: They should have their own cone beam machine or immediate access to one.
- Published research or lectures on zygomatic implants (indicates advanced expertise).
- A dedicated restorative dentist who works alongside the surgeon. Zygomatic implants require coordination between surgery and the final teeth.
Red Flags to Avoid
- A general dentist offering zygomatic implants without an OMFS on staff.
- No CBCT scan performed before scheduling surgery.
- Promises of “100% success guaranteed.”
- Refusal to show before-and-after photos of their own cases (not stock photos).
- Rushing you to book surgery without a second consultation.
Questions to Ask During Your Consultation
- “How many zygomatic implant surgeries have you performed in the last 12 months?”
- “What is your failure rate for zygomatic implants?”
- “Do you use 3D-printed surgical guides?”
- “What happens if an implant fails on my case? Who pays for the replacement?”
- “Can I speak with two or three of your past zygomatic patients?”
- “Do you have malpractice insurance that specifically covers zygomatic implants?”
Life After Zygomatic Implants: What to Expect Long-Term
Getting the implants is just the beginning. Your long-term success depends on good habits and regular maintenance.
The First Month After Surgery
- Week 1: Soft, cool foods (smoothies, pudding, mashed potatoes, soup). Ice packs on cheeks for 20 minutes on/20 minutes off. Sleep with your head elevated. Take prescribed pain medication as needed.
- Week 2: You can switch to warm soft foods (pasta, scrambled eggs, oatmeal). Swelling should be mostly gone. Start gentle salt water rinses after meals.
- Week 3–4: Most patients feel normal by now. You can eat soft bread, cooked vegetables, and tender fish. No biting with your front teeth yet. Use your bridge, but carefully.
Long-Term Maintenance (6+ Months)
Your permanent bridge (if zirconia) is very strong, but it is not indestructible.
Do’s:
- Brush twice daily with a soft toothbrush and non-abrasive toothpaste.
- Use a water flosser to clean under and around the bridge.
- Visit your dentist every 6 months for professional cleaning and exam.
- Wear a night guard if you grind your teeth (bruxism destroys implant bridges).
- Use a proxy brush or implant-specific floss to clean between the bridge and gums.
Don’ts:
- Do not chew ice, hard candy, or bones.
- Do not open packaging with your teeth.
- Do not smoke. Nicotine reduces blood flow to the bone and increases implant failure risk significantly.
- Do not skip cleanings. Plaque can build up and cause peri-implantitis (bone loss around the implant).
Lifespan of Zygomatic Implants
The titanium implants themselves can last 20+ years or even a lifetime if maintained well. The bridge on top wears out faster:
- Acrylic bridge: 5–10 years
- Zirconia bridge: 10–15+ years (often longer)
When the bridge wears down or breaks, your dentist can remove it, send it to a lab for repair or remake, and screw on a new one. The implants remain in place.
Common Myths About Zygomatic Implants
Let’s clear up some misinformation floating around the internet.
Myth #1: “Zygomatic implants are experimental.”
False. The first zygomatic implant was placed in 1988. They have been used clinically for over 35 years. The technique is well-studied, with hundreds of peer-reviewed papers confirming their safety and effectiveness.
Myth #2: “They make your cheekbones look bulky.”
False. The implant is inside the bone. It does not change the external contour of your face. No one will see or feel the implant through your skin.
Myth #3: “You can never have an MRI again.”
False. Titanium is non-ferromagnetic. You can safely have MRI scans with dental implants. You just need to inform the MRI technician, but it is rarely a problem.
Myth #4: “The surgery is extremely painful.”
Subjective. Any bone surgery causes postoperative discomfort. However, most patients report that zygomatic surgery is less painful than extensive bone grafting. The first 3 days are rough. By day 7, most people only need over-the-counter pain relievers.
Myth #5: “Anyone can place them with a weekend course.”
Dangerously false. Zygomatic implant placement requires advanced surgical training. Many countries require an oral and maxillofacial surgery residency (4–6 years after dental school) plus additional fellowship training. Do not trust a dentist who took a 2-day course.
Frequently Asked Questions (FAQ)
1. Are zygomatic implants removable?
No. They are fixed in your bone. The bridge can be unscrewed by a dentist for repairs or cleaning, but you cannot remove it yourself.
2. How many zygomatic implants will I need?
Most full-arch cases use 2 zygomatic implants (one on each side) plus 2 regular implants in the front. Severe cases with zero bone in the front might need 4 zygomatic implants.
3. Can I get zygomatic implants on one side only?
Yes. If you are only missing teeth on one side of your upper jaw (for example, after an accident), a single zygomatic implant can support a bridge limited to that side.
4. Do zygomatic implants work if I have a cleft palate?
In many cases, yes. But you need a surgeon experienced with cleft defects. The anatomy is different, and special planning is required.
5. What is the age limit for zygomatic implants?
There is no strict upper age limit. Elderly patients have successfully received zygomatic implants if they are healthy enough for surgery. However, patients under 18 typically wait until facial growth is complete.
6. How soon after extraction can I get zygomatic implants?
In most cases, you do not need to wait. The surgery can be done immediately if there is active infection. If you have severe gum disease, your surgeon may treat that first, then place implants 3–6 months later.
7. Will I taste metal?
No. The titanium is buried inside bone and covered by your gum tissue and the bridge. No metal touches your tongue or palate.
8. Can I get zygomatic implants if I smoke?
Yes, but with strong warnings. Smokers have significantly higher failure rates. If you cannot quit, your surgeon may still proceed, but you need perfect hygiene and more frequent follow-ups.
9. Do zygomatic implants interfere with speaking?
Initially, any new dental prosthesis feels bulky. After 1–2 weeks, your tongue adapts. Patients report that zygomatic-supported bridges restore normal speech better than removable dentures, which often slip and cause clicking sounds.
10. What happens if one zygomatic implant fails?
Your surgeon will assess the failed implant. It might be left in place (if stable but not integrated) and a new implant placed next to it. In the worst case, the bridge can be modified to work with the remaining implants.
Conclusion (Three Lines)
Zygomatic dental implants provide a proven, bone-graft-free solution for patients with severe upper jawbone loss. When placed by an experienced oral surgeon, they offer fixed, natural-looking teeth in a fraction of the time required for traditional grafting approaches. While the cost and complexity are higher than standard implants, the dramatic improvement in quality of life makes them a life-changing option for the right candidate.
Additional Resource
For a deeper dive into scientific studies and worldwide treatment protocols, visit the Zygomatic Implant Society’s patient education page:
🔗 www.zygomaticimplantsociety.org/patient-info
This resource offers a directory of certified surgeons, peer-reviewed research summaries, and a patient forum where you can read real experiences.
Disclaimer: This article is for informational purposes only and does not constitute medical or dental advice. Zygomatic implant surgery carries risks, including but not limited to infection, nerve injury, sinus complications, and implant failure. Always seek the advice of a qualified oral and maxillofacial surgeon with specific experience in zygomatic implants. Individual results vary. Do not disregard professional medical advice based on anything you have read here.