Bad Dental Implants: How to Spot, Survive, and Fix a Dental Nightmare
You saved up. You did your research. You sat through hours of surgery. And now? Something feels terribly wrong.
Bad dental implants are more common than most clinics want to admit. They don’t always mean you did something wrong. Sometimes the implant fails. Sometimes the dentist makes a mistake. And sometimes your body simply says “no” to a foreign object.
Whatever the reason, you are not alone. And more importantly, this is not the end of the road.
In this guide, we will walk through every red flag, every health risk, and every practical solution. No fluff. No scare tactics. Just honest, useful information to help you take back control.

What Exactly Counts as a “Bad” Dental Implant?
Let’s get clear on definitions first.
A good dental implant feels natural. It does not hurt. It does not move. You forget it is even there.
A bad dental implant is the opposite. It announces its presence constantly. Through pain. Through swelling. Through a bad taste in your mouth. Through the quiet but constant fear that something inside your jaw is going wrong.
Bad implants fall into three main categories:
- Biologically failing implants: Your body rejects the implant or develops an infection around it.
- Mechanically failing implants: The crown, abutment, or screw breaks or loosens.
- Poorly placed implants: The implant sits at the wrong angle, depth, or position from day one.
Each category has different causes, symptoms, and solutions. Let’s break them down.
Biologically Failing Implants
This is when your body fights the implant. The most common culprit is peri-implantitis—an inflammatory disease that destroys the bone and gum tissue around the implant.
Think of it as gum disease’s angrier cousin. Regular gum disease affects natural teeth. Peri-implantitis attacks the very foundation holding your implant in place.
Other biological issues include:
- Allergic reactions to titanium (rare, but real)
- Nerve damage during surgery
- Poor bone quality that cannot support the implant long-term
Mechanically Failing Implants
Sometimes the implant body itself is fine. The problem is the parts attached to it.
The implant is a three-part system:
| Component | Function | Common Failure |
|---|---|---|
| Implant post (screw) | Fuses with jawbone | Loosens or fractures |
| Abutment | Connects post to crown | Stripped threads or corrosion |
| Crown | The visible tooth | Chips, cracks, or falls off |
Mechanical failures produce distinct symptoms. You might hear a clicking sound when you chew. The crown might spin slightly. Or you might break a piece of the porcelain without any warning.
Poorly Placed Implants
This one stings because it is almost always the dentist’s fault.
An implant needs specific positioning. Too close to a nerve? You get chronic numbness or shooting pain. Too close to another tooth? You trap food and bacteria. Too shallow? The crown looks too long. Too deep? The crown looks short and food packs around it.
Poor placement does not always hurt immediately. Sometimes the problems take months or years to surface. But once they do, they rarely fix themselves.
Important note: A bad implant is not always visible to the naked eye. You can have a “perfect looking” crown that hides a failing implant underneath. Never judge success by appearance alone.
Red Flags: 12 Warning Signs You Should Never Ignore
Your body sends signals. Learning to read them early can save your implant—and your jawbone.
Here is a checklist of warning signs. If you check three or more boxes, call a different dentist for a second opinion.
Pain Signals
- Sharp pain when biting down
Not dull ache. Sharp. Like biting on a rock. This often means a loose abutment or cracked implant component. - Spontaneous throbbing
Pain that starts without any trigger. Especially at night. This suggests active infection or nerve involvement. - Pain that spreads to your ear, jaw, or temple
Implants in the lower jaw can refer pain along the trigeminal nerve pathway. Do not assume it is just TMJ.
Physical Changes
- Visible gum swelling or redness
Healthy gums around an implant should look pink and flat. Red, puffy, or purple gums are a hard no. - Bleeding when you brush or floss
Natural teeth bleed when inflamed. Implants should never bleed. Ever. - A bad taste or smell coming from the implant site
This is the hallmark of peri-implantitis. Bacteria are literally rotting the tissue around your implant. - The crown feels loose or moves
Even slight movement is abnormal. A healthy implant does not budge. - Receding gums around the implant
When the metal post becomes visible above the gum line, you are losing bone support.
Functional Problems
- Food constantly gets trapped around that tooth
Poor implant contours or incorrect positioning create open spaces where food packs like a trap. - You cannot floss between the implant and the adjacent tooth
The contact point should be snug but flossable. If floss snaps or shreds, something is wrong. - A clicking or squeaking noise when you chew
Metal-on-metal friction. Usually means two components are rubbing instead of staying tight. - Your bite feels “off” or uneven
You find yourself chewing only on one side. Or your jaw shifts to avoid hitting the implant.
When to Seek Immediate Help
Do not wait for your next cleaning appointment if you experience:
- Sudden swelling reaching your eye or neck
- Fever along with implant pain
- A loose implant that rocks back and forth
- Numbness in your lip, chin, or tongue that is new or worsening
These are urgent situations. Treat them like a broken bone or a bad infection. Because that is exactly what they might be.
The Real Health Risks of Leaving Bad Implants Alone
Ignoring a bad implant does not make it go away. It makes it worse. Sometimes dangerously worse.
Here is what actually happens inside your jaw when a failing implant stays put.
Bone Loss (The Silent Destroyer)
Your jawbone needs stimulation to stay strong. Natural teeth provide that stimulation through chewing. Implants provide it too—when they are healthy.
But a failing implant with active infection does the opposite. The infection eats away at bone. Month by month. Year by year.
The result? You lose bone volume. Not just around the implant. Sometimes entire sections of your jaw thin out to the point where a new implant becomes impossible without major bone grafting.
And you cannot grow jawbone back on your own. Once it is gone, restoring it means surgery. Big surgery.
Chronic Infection That Spreads
Peri-implantitis is not polite. It does not stay contained.
The bacteria surrounding a bad implant can:
- Spread to adjacent natural teeth (causing cavities and gum disease)
- Travel through your bloodstream (increasing inflammation throughout your body)
- Colonize other implants in your mouth
Research links long-term oral infections to heart disease, poorly controlled diabetes, and even pregnancy complications. A bad implant is not just a dental problem. It is a whole-body problem.
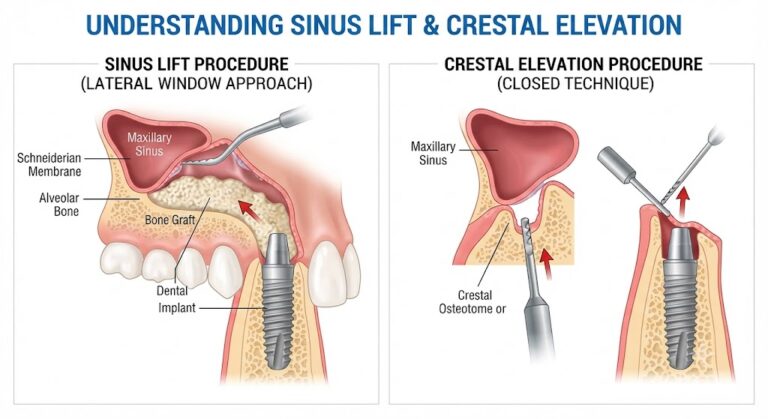
Sinus Involvement (Upper Jaw Implants)
Implants in the upper back jaw sit directly under your sinus cavity—the air-filled space behind your cheekbone.
A poorly placed or infected implant can:
- Perforate the sinus floor
- Push bacteria into the sinus
- Cause chronic sinusitis that never fully responds to antibiotics
You end up treating “sinus infections” for years when the real culprit is a bad implant sitting inches away.
Nerve Damage That Becomes Permanent
Some implant-related nerve damage heals. Most does not.
If an implant compresses or injures the inferior alveolar nerve (the main nerve in your lower jaw), you can experience:
- Permanent numbness in your lower lip, chin, and gum
- Chronic burning or tingling (like your face is asleep but also on fire)
- Drooling because you cannot feel when saliva escapes
- Difficulty speaking or pronouncing certain sounds
Once the nerve is severed or crushed, no surgery can fully repair it. Prevention is the only real cure.
Psychological Toll
Let’s be honest about the mental side.
Living with a bad dental implant is exhausting. You worry about every bite of food. You avoid smiling in certain lighting. You feel angry at the dentist who did this. And you feel stupid for trusting them.
These feelings are normal. And valid.
But do not let shame keep you from seeking help. Bad implants happen to careful, intelligent people every single day. The only mistake is pretending everything is fine.
Why Do Bad Implants Happen? (It’s Not Always Your Fault)
Let’s clear up a major source of guilt.
Many patients assume a failing implant must be their fault. “Did I brush wrong? Chew too hard? Skip a flossing session?”
Stop that.
While patient factors do play a role, most bad implants result from clinical errors or biological bad luck.
Clinical Errors (The Dentist’s Responsibility)
These are the hardest to accept because you trusted someone with your health and money.
- Insufficient bone assessment – Placing an implant without enough bone volume guarantees long-term failure. A CBCT scan (3D X-ray) should be mandatory. Any dentist placing implants without it is cutting corners.
- Poor angulation – An implant tilted even 10 degrees off the correct axis creates abnormal chewing forces that eventually break something.
- Overheating the bone – Drilling without enough irrigation kills bone cells. The implant goes in looking fine, but the bone never integrates properly.
- Contaminated implant surface – Touching the implant with gloves, saliva, or instruments before placement introduces bacteria that lead to early infection.
- Wrong implant size – Too narrow? Fracture risk. Too short? Poor stability. Too wide? Cracked jawbone. Size matters.
Patient Risk Factors (Your Responsibility)
These do not make the implant failure “your fault.” But they do influence your odds of success.
| Risk Factor | Impact on Implant Success |
|---|---|
| Smoking | Severely reduces blood flow and healing. Failure rate doubles. |
| Uncontrolled diabetes | Impaired immune response. Higher infection risk. |
| Osteoporosis medications (bisphosphonates) | Can cause jawbone death (osteonecrosis) after implant placement. |
| Gum disease history | Bacteria from remaining teeth easily infect new implants. |
| Teeth grinding (bruxism) | Creates excessive forces that loosen or fracture implants. |
| Poor oral hygiene | Plaque buildup directly causes peri-implantitis. |
Biological Bad Luck
Sometimes everything is done correctly. You follow all the rules. And the implant still fails.
- True titanium allergy – Rare (0.6% of patients). But real. Symptoms include chronic inflammation, skin rashes, or eczema flare-ups.
- Foreign body reaction – Some immune systems simply reject any implant, no matter how biocompatible.
- Unidentified bone pathology – Underlying bone diseases like fibrous dysplasia only become apparent after an implant fails.
In these cases, no one is to blame. But you still need a solution.
The Timeline: When Do Bad Implants Usually Show Themselves?
Not all bad implants fail on the same schedule. The timing tells you a lot about the cause.
Early Failures (0-4 Months)
These happen before the implant fuses with your bone. The bone never attaches properly.
- Typical timing: First 8-16 weeks after surgery
- Symptoms: Increasing pain, mobility, infection
- Most likely cause: Overheating, contamination, poor bone quality, or patient health factors
Early failures are actually good news in disguise. The implant comes out easily. Bone heals quickly. You can try again in 3-6 months.
Mid-Term Failures (4 Months – 2 Years)
The implant integrates initially. Then something goes wrong.
- Typical timing: Between crown placement and the second year
- Symptoms: Bone loss visible on X-rays, gum inflammation, bleeding
- Most likely cause: Bacterial infection (peri-implantitis), excessive chewing forces, or poorly fitting crown
Mid-term failures hurt more emotionally. You thought you were safe. But treatment is still very possible.
Late Failures (2+ Years)
These implants looked perfect for years. Then suddenly… problems.
- Typical timing: Any time after two years
- Symptoms: Gradual bone loss, crown loosening, implant fracture
- Most likely cause: Long-term peri-implantitis, bruxism, or mechanical fatigue
Late failures are the hardest to treat because significant bone loss may already exist. But modern dentistry has options. We will cover them.
Can a Bad Implant Be Fixed? Your Repair Options Explained
Good news. Many bad implants can be saved. Even some that feel hopeless.
The right repair depends entirely on what is wrong. Here is your decision tree.
Option 1: Non-Surgical Management (For Early Peri-Implantitis)
If you catch peri-implantitis very early—before major bone loss—you may avoid surgery.
What this looks like:
- Deep cleaning around the implant with special plastic instruments (metal scratches implant surfaces)
- Laser therapy to disinfect deep pockets
- Antibiotic gels or systemic antibiotics
- Intensive home care training
Success rate: Good for pockets less than 5mm deep with minimal bone loss. Poor if infection is advanced.
Option 2: Surgical Debridement (For Moderate Peri-Implantitis)
When pockets exceed 5mm or bone loss is visible, surgery becomes necessary.
The dentist:
- Lifts your gum tissue to expose the implant threads
- Cleans every contaminated surface
- Removes infected granulation tissue
- Places bone graft material into defects
- Sutures the gum back in place
Success rate: Approximately 70-80% when done correctly. Higher with strict follow-up care.
Option 3: Implant Component Replacement
If the implant body is healthy but the parts attached are broken, you only need a component swap.
Common component repairs:
- Tightening a loose abutment screw – Takes five minutes with a torque wrench
- Replacing a fractured crown – New crown fabricated from fresh impressions
- Changing a stripped abutment – Minor procedure under local anesthesia
These are simple fixes. No bone surgery. No implant removal. Just new parts.
Option 4: Implant Removal (When Saving Is Not Worth It)
Sometimes you need to cut your losses.
Indications for removal:
- Peri-implantitis destroying more than 50% of supporting bone
- Implant fracture below the gum line
- Nerve symptoms that worsen when the implant stays
- Patient chooses removal over ongoing maintenance
Removal sounds scary. In reality, it is usually straightforward.
How removal works:
Most implants unscrew backwards (counterclockwise) like a bolt. The dentist uses a special reverse-threaded tool. In five to fifteen minutes, the implant comes out.
For truly fused or fractured implants, a more invasive removal may be needed. But that is rare.
After removal, your bone heals for three to six months. Then you decide: new implant, bridge, or partial denture.
Option 5: Explant and Immediate Replacement
The most advanced option. Remove the bad implant and place a new one in the same appointment.
Requirements:
- Enough bone volume for a new implant
- No active infection
- Experienced surgeon with specialized tools
Not everyone qualifies. But when you do, it saves months of healing time and an extra surgery.
How to Find a Dentist Who Can Actually Fix Bad Implants
Not every dentist can fix someone else’s mistakes. You need specific skills.
The Right Credentials
Look for these specialists:
| Specialist | What They Do Best |
|---|---|
| Oral surgeon | Removing failed implants, nerve injuries, complex bone grafting |
| Periodontist | Treating peri-implantitis, gum surgery, implant maintenance |
| Prosthodontist | Fixing broken crowns and abutments, rebuilding bites |
Your regular general dentist is wonderful for cleanings and fillings. But bad implants often need a specialist’s hands.
Questions to Ask Before Booking
Call the office. Ask these exact questions:
- “How many failed implants from other offices do you treat each month?”
(A good answer is 5+ monthly. A no or “rarely” means they lack experience.) - “Do you have a CBCT scanner in-office?”
(If not, how can they diagnose bone loss and nerve position?) - “What percentage of your implant cases involve peri-implantitis treatment?”
(High volume means real experience.) - “Will you show me before-and-after photos of similar failed implants you have saved?”
(Visual proof beats promises every time.) - “Do you work with dental labs that specialize in implant restorations?”
(Generic labs produce generic results. Bad fits cause failures.)
Red Flags in a “Fixing” Dentist
Walk away if they:
- Promise to save every implant (unrealistic)
- Recommend removing a failing implant without imaging (reckless)
- Refuse to share X-rays or records with you (hiding something)
- Push expensive treatment on the first visit without explaining options (selling, not treating)
You need a partner, not a salesperson. Take your time.
Legal and Financial Options: When Someone Else’s Mistake Costs You
You paid for a working implant. You got a nightmare. What can you actually do about it?
Your Legal Rights
In most places, dental implants fall under medical malpractice or dental negligence laws. But here is the uncomfortable truth: proving a case is hard.
You must show:
- The dentist owed you a duty of care (yes, they did)
- The dentist breached that duty (they did something wrong)
- The breach directly caused your injury (not just bad luck)
- You have measurable damages (medical bills, lost time, pain)
The hardest part is #2. Some failures happen despite perfect care. You need an expert witness—another implant dentist—to testify that the original dentist violated the standard of care.
Before contacting a lawyer:
- Gather all records (X-rays, consent forms, treatment notes, receipts)
- Take dated photos of your implant site
- Document every symptom with dates and descriptions
- Get a second opinion in writing from an independent dentist
Important limitation: Most jurisdictions have a 2-3 year statute of limitations from the date you discovered (or should have discovered) the problem. Do not wait.
Financial Recourse Without Lawsuits
Legal action is stressful and expensive. Consider these alternatives first.
Dispute the credit card charge. If you paid by credit card and the treatment was clearly negligent, file a chargeback. Many patients win when they provide expert opinions.
File a board complaint. State dental boards investigate misconduct. They rarely refund your money. But a finding against the dentist strengthens future lawsuits. And it protects other patients.
Negotiate directly. Write a calm, factual letter to the dentist. State the problem. Attach supporting evidence. Propose a solution: full refund, free repair by a specialist, or partial settlement. Some dentists agree just to avoid bad reviews and board complaints.
Leave honest reviews. Google, Yelp, Healthgrades, RealSelf. Stick to facts. Describe what happened. Attach X-rays or photos. Future patients rely on these reviews. And unethical dentists sometimes reach out to resolve issues when public reputation is threatened.
Can Insurance Help?
Dental insurance rarely covers implant failures caused by negligence. Medical insurance sometimes covers infection treatment or nerve injuries.
Check your medical policy for:
- Surgical removal of a failed implant (covered as an oral surgery procedure)
- Hospitalization for severe infection
- Nerve injury treatment
Call your medical insurance directly. Ask: “Is the surgical removal of a failed dental implant covered if I have a documented infection or nerve injury?” Get the answer in writing.
Preventing Future Implant Failures: A Second Chance Strategy
If you get a second implant—or even if you keep your first one—do things differently this time.
The Pre-Implant Checklist Before Any New Surgery
Use this checklist before agreeing to any future implant placement.
- CBCT scan taken and reviewed with me
- Bone quality and quantity confirmed adequate for implant
- Existing gum disease treated and resolved
- Smoking cessation plan in place (at least 2 weeks before and 8 weeks after)
- Medical conditions optimized (A1c below 7 for diabetics)
- Nightguard fabricated if I grind my teeth
- Second opinion obtained from an independent implant specialist
Do not feel rude. Any confident dentist welcomes these questions.
The Maintenance Protocol That Actually Works
Healthy implants last decades. Unhealthy implants last years. The difference is maintenance.
Daily home care:
- Soft-bristle toothbrush (never metal or hard plastic on implant surfaces)
- Water flosser on low setting, angled into the gum pocket
- Implant-specific floss or superfloss with a stiffened end
- No abrasive toothpaste (it scratches titanium and attracts bacteria)
Professional maintenance schedule:
- Every 3-4 months for patients with peri-implantitis history
- Every 6 months for low-risk patients
- Annual CBCT to measure bone levels (X-rays alone miss early changes)
Warning: Regular hygienists can damage implants. Request a hygienist trained in implant maintenance. Plastic scalers only. No metal instruments. No ultrasonic scalers on titanium surfaces.
A Note on Monitoring at Home
Buy a simple periodontal probe online (do not actually probe yourself—leave that to a professional). But you can feel:
- Run a fingernail around the gum margin. Rough texture? That could be exposed implant threads from bone loss.
- Smell your floss after using it around the implant. Any odor? Infection.
- Look in a mirror. Can you see the edge of the metal post? Recession.
Check monthly. Keep a log. Early detection saves implants.
Real Patient Scenarios (Based on True Cases)
Let’s walk through three common stories. See which one sounds like you.
Scenario 1: The “It Never Felt Right” Case
Patient: Sarah, 42. One implant placed in a lower molar spot.
Symptoms from month two: Chronic dull ache. Could not chew on that side. The crown always felt “too high.” Her dentist adjusted the bite five times. Nothing helped.
What was actually wrong: The implant was placed too close to the inferior alveolar nerve. Not touching—but close enough that inflammation swelled the nerve. The implant itself was healthy. The position was just wrong.
Solution: Removal of the implant (the nerve symptoms stopped within three weeks). Bone graft. Six months later, a new implant placed by an oral surgeon using 3D-guided surgery. Perfect result. Sarah cried happy tears.
Lesson: Trust your gut. If it never feels right, get a second opinion before your first year is up.
Scenario 2: The “Hidden Infection” Case
Patient: Marcus, 58. Two implants supporting a three-tooth bridge in his upper jaw.
Symptoms: None for four years. Then his wife noticed his breath smelled bad. Marcus ignored it. A year later, the bridge wobbled. X-rays showed 70% bone loss around both implants.
What was actually wrong: Silent peri-implantitis. No pain because nerve endings were destroyed. But bacteria were eating his bone the entire time.
Solution: Both implants removed. Significant bone graft from his hip. A removable partial denture for two years. Finally, new implants. Marcus wishes he had come in as soon as his wife mentioned the smell.
Lesson: Bad breath that flossing and brushing do not fix equals infection until proven otherwise.
Scenario 3: The “Mechanical Mayhem” Case
Patient: Linda, 34. An implant in her front tooth position (the most visible spot).
Symptoms: The crown fell off three times in two years. Each time, her dentist glued it back. Cement kept squirting out from under the gum. Linda stopped smiling.
What was actually wrong: The abutment screw was cross-threaded from day one. It never tightened fully. The dentist’s “solution” of more cement only made things worse by trapping bacteria.
Solution: New abutment. New crown. A single torque wrench turned to 35 Ncm. The problem vanished. Linda spent $800 instead of $8,000 on new implant.
Lesson: Sometimes the implant is fine. The parts attached to it are junk. Get a second opinion from a prosthodontist before removing anything.
Summary Comparison: Good vs. Bad Dental Implants
| Feature | Good Implant | Bad Implant |
|---|---|---|
| Pain | None | Dull, sharp, or throbbing |
| Mobility | Zero movement | Wobbles or spins |
| Gum health | Pink, firm, no bleeding | Red, swollen, bleeds easily |
| Bone level | Stable or minimal loss over time | Progressive loss on X-rays |
| Chewing function | Normal | Painful or avoided |
| Maintenance | Routine cleaning | Frequent infections and repairs |
| Long-term prognosis | 95% success at 10 years | Guarded to hopeless |
Additional Resource
For peer-reviewed research on peri-implantitis prevalence and treatment outcomes, visit the American Academy of Periodontology’s clinical guidelines page (search “AAP peri-implantitis guidelines”).
Frequently Asked Questions (FAQ)
Q: Can a bad dental implant make me sick overall?
Yes. Chronic oral infections from failed implants increase systemic inflammation. Links exist to heart disease, diabetic complications, and even pneumonia from aspirated bacteria.
Q: How long can I leave a bad implant in my mouth?
Not long. Every month you wait, you lose more bone. After six months of active infection, you may need major bone grafting to place a new implant. Remove it earlier to preserve your options.
Q: Will my dental insurance cover implant removal?
Sometimes. Many plans cover “extraction of a failed dental implant” under oral surgery benefits. Call your provider and ask for the specific code (usually D6100 or D6190). Medical insurance rarely covers removal unless infection or nerve injury exists.
Q: Is it worth suing my dentist for a bad implant?
Only if you have clear negligence evidence: wrong placement visible on X-rays, no pre-surgical CBCT scan when needed, or documented refusal to treat complications. For average failures, legal fees often exceed any settlement. Consult a dental malpractice attorney for a free case review first.
Q: Can I get a new implant in the same spot?
Yes, in most cases. After removing the bad implant, your bone needs 3-6 months to heal. Then a surgeon reassesses bone volume. If enough remains, a new implant goes in. If not, bone grafting first, then implant.
Q: Do cheap dental implants fail more often?
Not necessarily. Brand matters less than surgical skill and your own health. A cheap implant placed perfectly has a better chance than an expensive implant placed poorly. That said, discount clinics often cut corners on imaging, sterilization, and follow-up care.
Q: Why does my implant hurt when I have a sinus infection?
Upper implants sit under your sinus floor. Sinus inflammation pushes down on the implant tip. That pressure hurts because the implant is rigidly fixed—unlike natural teeth, it cannot “give” slightly. Treat the sinus infection, and the implant pain usually stops.
Conclusion: Your Path Forward
Bad dental implants are physically painful, emotionally draining, and financially frustrating. But you have real options. Catch the warning signs early. Find a specialist who fixes other dentists’ mistakes. Remove or repair before bone loss spreads. And build a maintenance plan that protects your second chance. You can absolutely get your smile back.