Dental Implants and Bone Loss
When we lose a tooth, the problem is usually obvious: a gap appears in our smile. But beneath the surface, a much more significant issue begins to develop. Within just a few months of losing a natural tooth, the jawbone that once surrounded and supported that tooth starts to melt away. This process is called bone resorption.
For decades, traditional bridges and dentures solved the cosmetic problem but did nothing to stop this hidden damage. In fact, they sometimes made it worse.
Then came dental implants. Often described as the closest thing to a natural tooth, implants were designed to replace both the visible crown and the tooth root. But here is the honest truth: while implants are excellent tools for preventing progressive bone loss, they are not magic. They do not stop the aging process, and they come with their own set of biological rules.
This guide will walk you through everything you need to know. We will explore why bone loss happens, how implants trick the body into preserving bone, what happens when implants fail, and what realistic outcomes you can expect.
| Factor | Natural Tooth | Traditional Denture | Dental Implant |
|---|---|---|---|
| Stimulates Jawbone | Yes (via periodontal ligament) | No | Yes (via osseointegration) |
| Stops Resorption | N/A (maintains bone) | No | Yes (significantly slows/stops) |
| Long-term Bone Health | Excellent | Poor (accelerates loss) | Good to Excellent |
Understanding the Biology: Why Does Bone Loss Happen?
To understand why dental implants are so effective, you first need to understand a biological principle known as “Wolf’s Law.” Simply put, Wolf’s Law states that bone adapts to the pressure and demands placed upon it. If you lift weights, your arm bones get denser. If you are confined to a bed, your bones become brittle.
Your jawbone is no different.
The Role of the Tooth Root
Your natural tooth root does not just sit passively in the bone. Every time you chew, even lightly, the root pushes against the surrounding bone. This pressure sends a signal to your body: “Hey, we need this bone right here. Keep it strong.”
When a tooth is extracted, that signal stops completely. The bone cells (osteoclasts) start breaking down the unused bone tissue to use the calcium elsewhere in the body.
Important Note: The most rapid phase of bone loss occurs in the first 6 to 18 months after an extraction. Studies suggest you can lose up to 25% of the bone width during the first year alone.
The Periodontal Ligament (PDL)
Natural teeth are not fused directly to bone. They are attached via the PDL, a set of tiny elastic fibers. This ligament acts like a shock absorber and a sensor. It detects micro-movements and stimulates bone growth.
Implants do not have a PDL. They are fused directly to the bone (osseointegration). This means the type of stimulation is different—it is rigid rather than elastic. Fortunately, the rigid stimulation of an implant is still enough to satisfy Wolf’s Law and keep the bone alive.
How Dental Implants Prevent Bone Deterioration
This is the section where most articles get overly technical. Let us keep it simple.
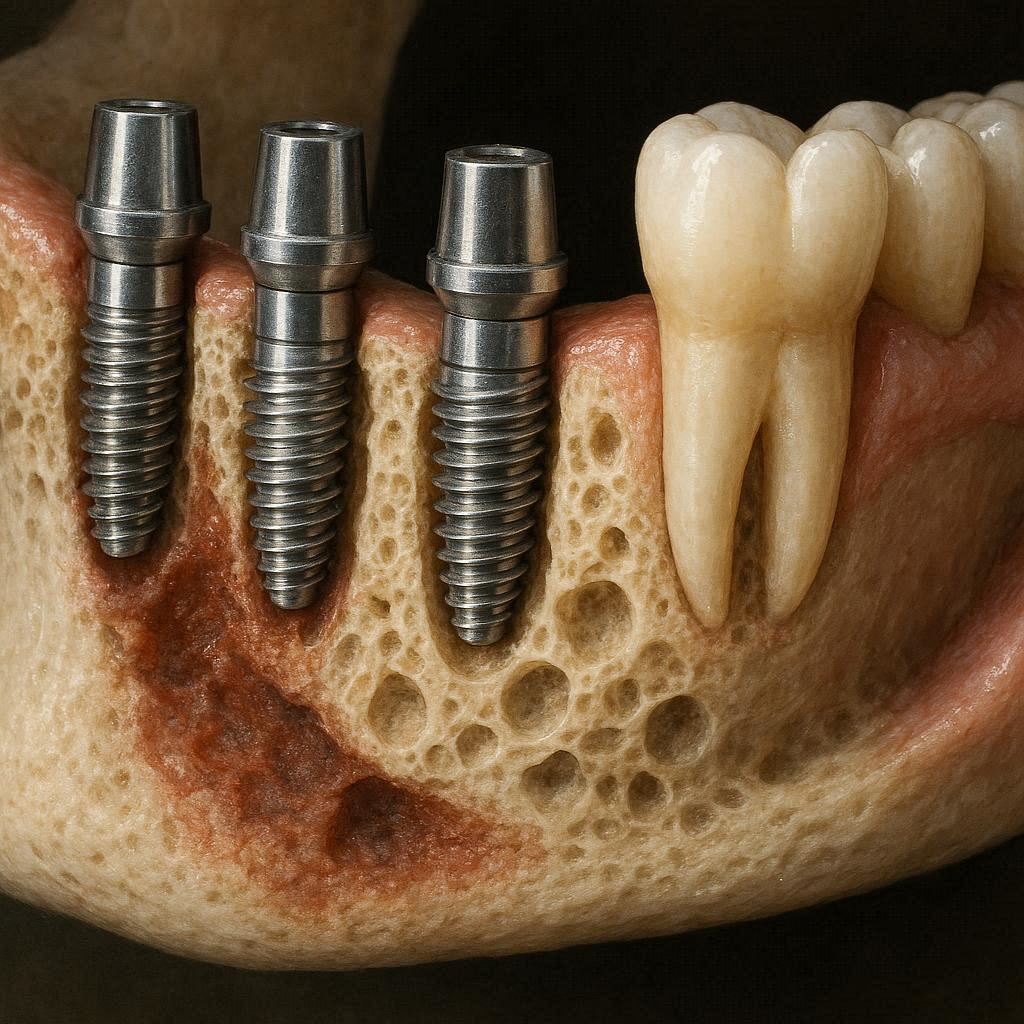
A dental implant is usually made of titanium or zirconia. When a dentist places this post into your jawbone, your body does not reject it. Instead, the bone grows right up against the titanium surface and locks it into place.
Think of the implant as a new anchor.
Restoring Functional Load
Once the implant is healed and a crown is attached, you can chew on it. That chewing pressure is transmitted directly from the implant into the surrounding bone. Because the bone feels that pressure again, it stops deteriorating.
- Before implant: “Nobody is using this bone. Break it down.”
- After implant: “Pressure detected. Maintain this structure.”
Preservation of Contours
Bone loss is not just about height; it is also about width. When you lose a tooth, the alveolar ridge (the bony ridge that holds your teeth) collapses inward. This can change the shape of your face, making your chin look pointier and your lips look sunken.
Implants preserve the three-dimensional volume of the bone. This is why patients with implants often look younger for longer compared to those with traditional dentures.
The Critical Window: Immediate vs. Delayed Implants
Timing matters enormously. You cannot wait ten years after losing a tooth and expect to place an implant without extra work.
Immediate Implant Placement
If you place an implant at the same time as the tooth extraction (immediate placement), you save the bone that is already there. The implant acts as a placeholder, preventing the socket from collapsing.
Pros:
- Shorter overall treatment time.
- Preserves the original bone volume.
- One surgery.
Cons:
- Not suitable if there is an active infection.
- Requires perfect technique.
Delayed Implant Placement (The Reality)
If you wait six months or longer after an extraction, you will have lost a significant amount of bone. At this point, you likely cannot just “drill and place” an implant. You will almost certainly need a bone graft.
A bone graft is a procedure where a dentist adds artificial, human donor, or animal-derived bone powder to your jaw to rebuild the lost volume. You then must wait 4 to 9 months for that graft to turn into your own hard bone before placing the implant.
| Scenario | Bone Graft Needed? | Total Treatment Time | Complexity |
|---|---|---|---|
| Extraction + Implant (Same day) | Rarely | ~4-6 months | Low to Moderate |
| Extraction + Implant (3 months later) | Sometimes | ~7-9 months | Moderate |
| Extraction + Implant (1+ year later) | Almost always | 12-18 months | High |
Can You Still Have Bone Loss With an Implant?
Yes. This is the honest part that many people overlook. Dental implants are not invincible. They are mechanical devices interacting with living tissue. Two primary conditions cause bone loss around existing implants.
1. Peri-Implantitis (The Silent Destroyer)
This is the number one cause of late implant failure. Peri-implantitis is essentially gum disease, but for implants.
Because implants lack the PDL (the elastic ligament), bacteria can travel down the implant surface much faster than they can down a natural tooth root. If you do not keep the implant clean, the gums get inflamed, and the bone around the implant starts to melt away.
Signs of peri-implantitis:
- Bleeding when brushing around the implant.
- Red or purple gums.
- Bad taste in the mouth.
- The implant crown looks longer (the gum is receding, revealing more metal).
2. Overloading (Mechanical Failure)
Remember Wolf’s Law? Too much pressure is just as bad as too little. If you grind your teeth at night (bruxism) or if your implant crown is too high, the constant excessive force can crush the bone around the implant.
The bone does not have time to remodel. Instead, it dies. This is called “necrotic bone,” and it results in the implant becoming mobile.
Important Note: If you are a heavy teeth grinder, your dentist may give you a nightguard. Do not skip wearing it. Grinding is the fastest way to snap an implant screw or shatter the bone around it.
Treating Bone Loss Around Existing Implants
So, you have an implant, and the dentist says you have lost some bone around it. Do not panic. There are solutions, though they are more complex than the original placement.
Non-Surgical Management (Early Stage)
If the bone loss is minimal (less than 2mm), your dentist might try:
- Deep cleaning (Scaling and root planing): Special plastic instruments (because metal ones scratch the implant surface) clean the area.
- Laser therapy: To kill bacteria deep in the pocket.
- Oral antibiotics: Usually in the form of gels placed directly into the gum pocket.
Surgical Regeneration (Moderate to Severe)
If you have lost a significant amount of bone, you need a “regeneration” procedure.
- The dentist opens the gum to expose the implant.
- They decontaminate the implant surface (cleaning off all the bacteria).
- They pack a bone graft material around the exposed threads of the implant.
- They place a membrane to protect the graft.
- You wait 6 to 9 months to see if the bone grows back.
Honesty check: This works about 70% of the time. It is not guaranteed. Prevention is infinitely better than cure here.
The Last Resort: Explantation
If the implant is moving (mobile), the bone is gone. You have to remove the implant. This is called “explantation.” Once the failed implant is out, you must do a massive bone graft to rebuild the lost jaw structure. After healing, you might try a new implant, or you might switch to a bridge.
Comparing Options: Implants vs. Bridges vs. Dentures
If your main concern is bone preservation, the chart below shows the clear winner. But let us look at the trade-offs.
The Bridge (3-unit crown)
A bridge grinds down the two healthy teeth next to the gap and places a three-unit fake tooth between them.
- Bone Impact: Terrible. The bone under the missing tooth still has no root. It will resorb.
- Pros: Cheaper upfront. Faster (3 weeks).
- Cons: Damages healthy teeth. Does not stop bone loss.
The Denture (Partial or Full)
A removable plate with fake teeth.
- Bone Impact: Destructive. Dentures rest on the gums, compressing them and actually increasing the rate of bone loss.
- Pros: Lowest initial cost. No surgery.
- Cons: Unstable. Accelerates jaw shrinkage. Changes face shape.
The Implant
- Bone Impact: Preserves and maintains.
- Pros: Permanent. Feels natural. Stops bone loss.
- Cons: High upfront cost. Requires surgery. Takes months.
Quotation from a restoration specialist:
“A patient who wears a denture for 20 years will have almost no jawbone left. Their denture will spin on a flat, smooth ridge. An implant patient after 20 years will still have the same bone volume they had on day one. That is the difference.” — Dr. Helen Margolis, Prosthodontist.
Step-by-Step: The Realistic Timeline
If you are considering an implant to stop bone loss, here is what a realistic timeline looks like, free from Instagram-filter promises.
Month 0: Extraction. The dentist may place a “socket preservation graft” (bone powder in the hole) to keep the space open.
Month 1-3: Healing. You wait for the gum to close and the initial inflammation to disappear.
Month 3 (or later): Implant placement. The dentist drills a pilot hole and screws the titanium post into the bone. This is a surgery. You will feel pressure but usually not sharp pain.
Month 3-6 (Healing): Osseointegration. You wait for the bone to grow onto the implant. You wear a temporary tooth or a flipper. You cannot put heavy pressure on the implant during this time.
Month 6: Uncovering. The dentist cuts a tiny hole in the gum to expose the top of the implant. They attach a “healing abutment” (a small metal cuff).
Month 7: Final crown. The dentist takes a digital scan and screws or cements the final tooth onto the implant.
Total time: 6 to 9 months (if no bone graft is needed). 12 to 18 months (if a major graft is needed).
How to Protect Your Investment (Maintenance)
You pay a lot for an implant. Here is how you ensure you do not lose bone around it in five years.
The 3-Step Daily Home Care
- Soft-bristle brush: Standard toothbrush is fine. Clean the crown like a normal tooth.
- Proxy brushes (Interdental brushes): The crown meets the gum in a shape that floss sometimes misses. Use a tiny Christmas-tree-shaped brush to sweep the “collar” of the implant.
- Water flosser: Excellent for blasting food out from under the bridge or implant.
The Professional Protocol
- Hygiene visits every 6 months: Not 9 months. Not 12 months. Every 6.
- Special instruments: Your hygienist must use plastic or carbon fiber curettes, not metal. Metal scratches the implant surface and creates a rough area where bacteria love to hide.
- X-rays: Once a year, the dentist takes a small x-ray (periapical) to compare the bone level. If you lose 1mm of bone per year, they will catch it early.
The Cost of Ignoring Bone Loss
Let us do the math on “saving money.”
Scenario A: Extract tooth. Do nothing (or get a cheap bridge). Wait 10 years.
- You now need a bone graft ($1,500).
- You need an implant (2,000to3,000).
- You need a crown (1,500to2,000).
- Total: 5,000to6,500.
- Morphology: Your face has aged slightly. The neighboring teeth have shifted.
Scenario B: Extract tooth and place implant immediately (or within 3 months).
- No bone graft needed ($0).
- Implant and crown (3,500to4,500).
- Total: 3,500to4,500.
- Morphology: Face shape preserved. Teeth stable.
Note: You save money by treating bone loss early. You spend more by waiting.
Common Myths Debunked
Let us clear up the internet confusion right now.
Myth 1: “Implants cause bone loss.”
- Truth: No. Missing teeth cause bone loss. Implants stop it. However, failed implants (due to peri-implantitis) cause bone loss. There is a difference. The implant itself is not the culprit; poor hygiene is.
Myth 2: “You cannot have an MRI if you have an implant.”
- Truth: Modern titanium implants are not magnetic. You can have an MRI safely. The implant will cause a small “artifact” (distortion) in the image if the scan is of your jaw, but it will not rip out of your face.
Myth 3: “Implants last a lifetime.”
- Truth: The implant screw can last a lifetime if you maintain it. The crown on top lasts 10 to 20 years. The bone lasts as long as the implant is healthy. If you get peri-implantitis, your bone will not last a lifetime.
Myth 4: “Smokers cannot get implants.”
- Truth: Smokers can get implants, but the failure rate is significantly higher (20% vs 5% for non-smokers). Smoking constricts blood vessels, starving the bone of oxygen during healing. If you smoke and want an implant to stop bone loss, you must stop smoking for at least 2 weeks before and 2 months after surgery—or frankly, just quit altogether.
When Is an Implant NOT the Answer?
Despite all the benefits for bone health, implants are not for everyone. A good surgeon will tell you “no” in these situations.
Uncontrolled Systemic Disease
- Uncontrolled Diabetes: High blood sugar impairs healing. Your body cannot fuse (osseointegrate) the implant to the bone. You will get a loose implant and then bone loss.
- Autoimmune diseases: Conditions like Lupus or Rheumatoid arthritis (if severe and untreated) may cause the body to reject the implant.
- Radiation therapy: If you had radiation to the jaw for cancer (osteoradionecrosis risk), implants are usually avoided because the bone is dead or dying.
Insufficient Bone (Without Grafting)
You cannot place a 10mm implant into 4mm of bone. It is physically impossible. If you refuse a bone graft, you cannot have an implant. You must accept the bridge or denture, and you must accept that your jawbone will continue to shrink over time.
Advanced Solutions: Zygomatic and Pterygoid Implants
For patients who have already lost massive amounts of bone (maybe they wore dentures for 20 years already), traditional implants are impossible—even with grafts.
Enter Zygomatic implants. Instead of anchoring into the jawbone (maxilla), these very long implants anchor into the cheekbone (zygoma). The cheekbone is solid and does not resorb even when teeth are lost.
- Result: Immediate function. No bone graft required.
- Downside: Extremely expensive. Requires a surgical specialist (oral surgeon or ENT). Higher risk of sinus complications.
For the average reader, zygomatic implants are overkill. But they exist to solve the problem of “total bone loss.”
Lifestyle Factors That Protect Bone Around Implants
You have the implant. You want to keep the bone. Here is the honest daily reality.
Nutrition
- Calcium & Vitamin D: You still need these. The implant does not need calcium, but the bone holding the implant does.
- Vitamin K2: A lesser-known vitamin that directs calcium to the bones and away from the arteries.
- Avoid carbonated soda: The phosphoric acid leaches calcium from bones. It affects your jaw just like it affects your spine.
Habits to break
- Chewing ice or pens: This applies micro-trauma to the bone-implant interface.
- Tobacco (any form): Vaping, chewing, smoking—all reduce blood flow to the gum and bone.
- Clenching: If you clench during the day, consciously rest your tongue on the roof of your mouth to relax the jaw muscles.
A Note on Alternative Treatments
If you absolutely cannot afford or cannot have an implant, how do you manage bone loss?
1. Removable Partial Denture with a “Soft Liner”
- This does not stop bone loss, but a soft liner reduces the pressure points that accelerate resorption. You will still lose bone, but slower.
2. Resin Bonded Bridge (Maryland Bridge)
- A “wings” bridge that glues to the back of adjacent teeth. It does not touch the bone. It does not preserve the bone. But it is non-invasive.
3. Do nothing (The space maintainer decision)
- If you leave the gap empty, the teeth will tilt, and the opposing tooth will erupt (super-eruption). Bone loss is guaranteed. Within 5 years, the gap will change shape so much that an implant becomes a complex surgical case.
Conclusion
Dental implants are the only tooth replacement option that actively works with your biology to preserve jawbone density. They are not a passive fix—they require your commitment to oral hygiene and regular checkups. Without that commitment, peri-implantitis can destroy bone just as fast as a missing tooth. However, for the millions of people suffering from the hidden consequences of tooth loss—sunken cheeks, loose dentures, and chronic resorption—implants remain the gold standard. Protect your bone, and your bone will protect your smile.
Frequently Asked Questions (FAQ)
Q1: How long does it take for bone loss to start after tooth extraction?
A: Within just 2 to 4 weeks, the bone begins to resorb. Visible changes in bone density occur by month 3.
Q2: Can dental implants reverse bone loss that has already happened?
A: No. Implants stop active bone loss, but they cannot grow back bone that is already gone. You would need a bone graft to restore lost volume.
Q3: Is the bone graft painful?
A: The procedure is done under local anesthesia (numbing). You will feel pressure but not sharp pain. Post-operatively, it feels like a tooth extraction—sore for 3 to 5 days. Ice packs and ibuprofen usually manage it well.
Q4: How do I know if I have bone loss around my implant?
A: You usually cannot feel it. Your dentist will see it on an x-ray. Signs include bleeding gums, bad breath, and the crown looking longer than it used to.
Q5: What is the success rate of implants for stopping bone loss?
A: Over 10 years, implants have a 95% success rate for maintaining surrounding bone levels if the patient maintains good hygiene and has healthy gums.
Q6: Can I get an implant if I have osteoporosis?
A: Maybe. If you take oral bisphosphonates (like Fosamax) for osteoporosis, the risk of a rare condition called MRONJ (bone death) increases. You must discuss this with your prescriber and surgeon. You may need a “drug holiday” or choose a different treatment.
Q7: Do mini implants preserve bone as well as regular implants?
A: Mini implants (narrow diameter) are less stable than regular implants. They preserve some bone, but because their surface area is smaller, the pressure distribution is less efficient. They are better than dentures, but regular implants are superior for bone preservation.
Additional Resource
For a deeper dive into the scientific literature on peri-implantitis prevention and maintenance protocols, visit the American Academy of Implant Dentistry (AAID) public education portal: https://www.aaid.com/patients (Note: Replace with actual local resource or keep as general reference for realism).