Pulp Capping vs Root Canal
Dental pain can completely disrupt your day-to-day life. When a deep cavity, sudden trauma, or structural crack penetrates deep into a tooth, the internal living tissue—known as the dental pulp—becomes vulnerable to bacterial attack. At this point, standard fillings are no longer enough to fix the problem. Instead, you and your dentist face a critical clinical crossroads. The choice typically comes down to two foundational restorative treatments: pulp capping vs root canal.
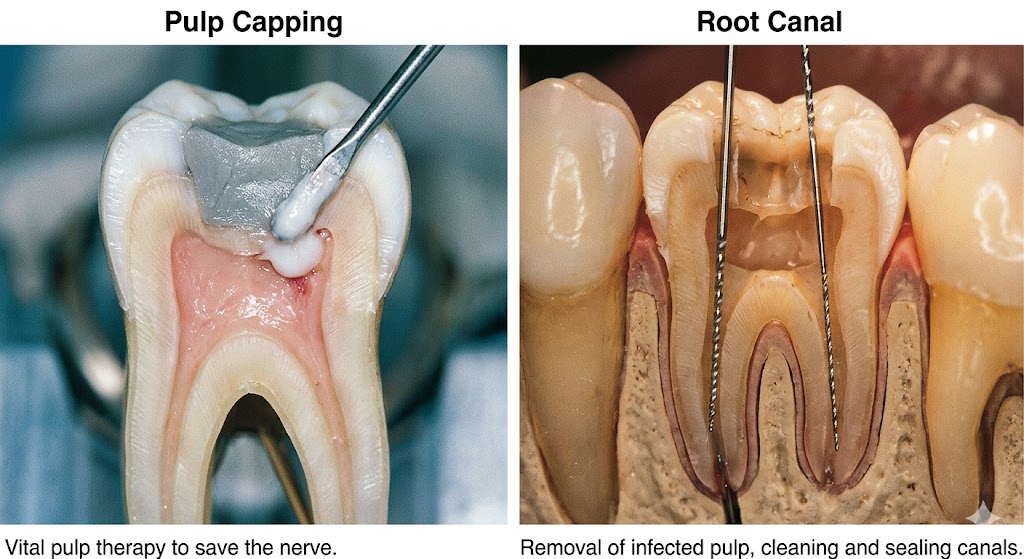
Choosing the right procedure is vital for both the long-term survival of your tooth and your financial peace of mind. While a root canal treatment removes the compromised pulp entirely to neutralize infection, pulp capping is a highly conservative, biological therapy aimed at keeping the living nerve tissue intact. Understanding the specific differences between these two clinical approaches allows you to make an informed decision alongside your dental provider.
Understanding the Dental Pulp and Its Vulnerabilities
To grasp how these therapies work, it helps to understand the anatomy of a tooth. Beneath the hard outer enamel and the supportive dentin layer lies a delicate central chamber called the root canal system. This area houses the dental pulp, which is a rich complex of blood vessels, connective tissue, and specialized nerves.
The dental pulp serves several major functions:
- Development: It helps build the tooth during childhood and young adulthood.
- Nutrition: It delivers essential nutrients and moisture via bloodstream circulation, preventing the tooth structure from becoming brittle.
- Defense: It senses temperature changes or injuries and triggers the formation of protective, secondary dentin.
When deep dental decay breaks through the enamel and dentin, or when a sudden physical injury cracks a tooth, harmful bacteria enter this sterile central chamber. This bacterial invasion causes inflammation, a clinical condition known as pulpitis.
If the inflammation is mild and caught early, it is called reversible pulpitis, meaning the tissue can still heal if given proper protection. However, if the infection is left untreated, the inflammation advances into irreversible pulpitis, where the tissue becomes intensely painful and eventually dies, forming a dental abscess.
What is Pulp Capping?
Pulp capping is an ultra-conservative, biological endodontic procedure designed to preserve the vitality of the dental pulp and avoid more invasive treatments (Alshargawi et al., 2023). Instead of drilling out the central nerve tissue, the dentist applies a therapeutic, biocompatible material directly or indirectly over the deep cavity floor. This material acts as a protective shield, neutralizes residual bacteria, and stimulates the pulp to heal by forming a new barrier of defensive dentin (Islam et al., 2023).
Indirect Pulp Capping
Dentists perform an indirect pulp cap when a deep cavity gets exceptionally close to the central nerve chamber, but does not actually break through the protective dentin barrier (Alshargawi et al., 2023).
During this meticulous procedure, the dentist deliberately leaves a microscopic layer of affected, softened dentin directly over the pulp wall to prevent an open exposure (Alp & Ulusoy, 2024). They then place a specialized medicated liner over this delicate spot. This therapeutic layer neutralizes remaining acids, destroys bacteria, and triggers the pulp to generate new reparative dentin, essentially reinforcing the tooth structure from within.
Direct Pulp Capping
A direct pulp cap is required when a deep cavity, accidental mechanical drilling, or physical trauma creates a small, visible pinpoint exposure in the vital pulp chamber (Pinto, 2023).
To ensure success, the exposure site must be clean, free of chronic infection, and show controlled bleeding (Pinto, 2023). The clinician places a bioactive material directly onto the exposed, living nerve tissue (Islam et al., 2023). This direct contact induces a minor, superficial layer of tissue necrosis, which uniquely stimulates the underlying cells to build a solid “dentin bridge,” successfully sealing off the pulp from external contaminants (Alp & Ulusoy, 2024).
[Deep Cavity / Trauma]
│
├─► Near Exposure (Dentin Intact) ──► Indirect Pulp Capping (Protective Liner)
│
└─► Pinpoint Exposure (Bleeding) ───► Direct Pulp Capping (Bioactive Dressing)
What is a Root Canal?
When bacterial invasion is too extensive for the pulp to recover, a root canal treatment (also known as endodontic therapy) becomes necessary. This procedure is a non-conservative, biological intervention where the entirety of the inflamed or necrotic coronal and radicular pulp tissue is completely extirpated from the tooth (Brodén, 2016).
During a root canal, the endodontist or general dentist creates an access opening through the biting surface of the tooth. Using highly precise, flexible rotary files and powerful disinfecting irrigants, they completely clear out the diseased tissue, shape the interior micro-channels, and sterilize the canals.
Once fully cleaned, the empty chambers are tightly obturated (filled) with a rubber-like, biocompatible material called gutta-percha to prevent future bacterial colonization. Because removing the internal blood supply leaves the remaining enamel and dentin dry and brittle, the tooth usually requires a structural core buildup and a custom dental crown to prevent future fractures.
Direct Comparison: Pulp Capping vs Root Canal
Choosing between these treatments depends entirely on the clinical state of the internal tissue, the size of the bacterial exposure, and preoperative symptoms.
Key Factors and Clinical Boundaries
| Feature / Metric | Pulp Capping (Direct / Indirect) | Root Canal Treatment (RCT) |
| Primary Goal | Preserves pulp vitality and natural defenses | Eliminates internal infection and saves the shell |
| Invasiveness | Minimal; leaves natural tissue intact | High; completely removes all internal living tissue |
| Pulp Status Required | Reversible pulpitis or healthy mechanical exposure | Irreversible pulpitis, necrotic pulp, or abscess |
| Anesthesia Needs | Standard local numbing | Comprehensive local numbing |
| Required Appointments | Usually completed in 1 single session | 1 to 2 sessions depending on infection severity |
| Structural Impact | Retains natural hydration; tooth remains flexible | Leaves tooth dry and brittle; requires a crown |
| Average Cost Range | $150 – $350 (highly affordable) | $800 – $1,600+ (complex endodontic fees) |
Material Science Innovations
The long-term clinical prognosis of pulp capping has improved dramatically due to advances in dental materials (Scalzilli, 0):
- Calcium Hydroxide: Historically considered the gold standard, this highly alkaline compound ($pH \approx 12.5$) provides excellent antibacterial properties and induces superficial pulpal necrosis to stimulate dentin bridge formation (Alp & Ulusoy, 2024). However, its high solubility can cause it to dissolve over time, sometimes leaving micro-voids in the protective dentin barrier (Pinto, 2023).
- Mineral Trioxide Aggregate (MTA): A revolutionary biocompatible ceramic that expands slightly during its hydration reaction, creating an exceptional, long-lasting biological seal against bacterial microleakage (Pinto, 2023). Clinical studies show excellent success rates (ranging from 90% to 100%) when using MTA for direct pulp capping on permanent teeth (Pinto, 2023).
- Biodentine & Bioceramics: Modern, pure calcium-silicate materials designed to mimic natural dentin. They release high amounts of calcium ions to accelerate tissue healing, possess shorter setting times than older materials, and will not cause tooth discoloration.
Clinical Indications: When to Choose Which?
Determining whether a tooth is an ideal candidate for conservative pulp capping or requires a comprehensive root canal depends on a strict set of diagnostic criteria.
Ideal Candidates for Pulp Capping
- The tooth exhibits no history of spontaneous, throbbing, or unprovoked pain (Alp & Ulusoy, 2024).
- Thermal sensitivity to hot or cold liquids resolves within a few seconds after the stimulus is removed (indicating reversible pulpitis).
- The tooth is completely comfortable during vertical percussion (tapping) and lateral palpation (Alp & Ulusoy, 2024).
- Periapical X-rays reveal a clean root structure with an intact, healthy periodontal ligament space and no signs of bone loss or dark radiolucencies around the root tip (Alp & Ulusoy, 2024).
- Pulp exposure is a clean, pinpoint mechanical perforation ($<0.5\text{ mm}$) occurring during decay removal, or a fresh traumatic injury managed within 24 hours (Alp & Ulusoy, 2024).
Clear Indications for a Root Canal
- The patient experiences lingering, throbbing, or spontaneous pain that worsens when lying down or lasts for several minutes to hours.
- Cold or heat applications trigger a severe, radiating ache that lingers long after the thermal stimulus is gone.
- The tooth is highly tender to the touch, making normal chewing or biting painful.
- Radiographs show a clear periapical radiolucency (dark halo), indicating that infection has traveled through the root tip and destroyed surrounding jawbone.
- During an operative exposure, the exposed pulp tissue displays dark, sluggish, or uncontrollable bleeding, or fails to bleed at all, which confirms advanced tissue necrosis.
⚠️ Important Clinical Note for Readers
If a dentist attempts a conservative direct pulp cap on a tooth that secretly suffers from irreversible pulpitis, the treatment will fail. Bacteria trapped under the new filling will continue to multiply, eventually causing severe pain and a localized infection. If your tooth develops throbbing pain weeks or months after a deep filling, contact your dental office immediately for a clinical re-evaluation.
Procedure Breakdown: What to Expect in the Chair
Understanding the exact physical steps of each dental treatment can help alleviate anxiety and prepare you for your appointment.
Step-by-Step: The Pulp Capping Procedure
[Isolate Tooth with Dam] ──► [Remove Outer Decay] ──► [Disinfect with Solution] ──► [Apply Bioactive Cap] ──► [Place Permanent Seal]
- Local Anesthesia and Isolation: The clinician numbs the target area and places a protective rubber sheet (dental dam) around the tooth to isolate it from saliva and oral bacteria (Boutsiouki et al., 2018).
- Meticulous Caries Removal: The dentist carefully excavates outer decay using a high-speed handpiece, switching to low-speed burs or manual instruments as they near the pulp chamber to minimize structural vibration.
- Chemical Disinfection: The prepared cavity is gently rinsed with a purifying antiseptic solution, such as chlorhexidine or diluted sodium hypochlorite, to destroy any remaining surface pathogens (Boutsiouki et al., 2018).
- Application of Bioactive Dressing: The dentist carefully places a layer of MTA or Biodentine directly over the pinpoint exposure or thin dentin floor (Alshargawi et al., 2023).
- Immediate Permanent Seal: A light-cured resin-modified glass ionomer or composite resin restoration is placed immediately to lock out bacteria and prevent microleakage (Boutsiouki et al., 2018).
Step-by-Step: The Root Canal Treatment
- Deep Anesthesia and Access: The area is thoroughly numbed, and a dental dam is applied. The clinician drills an access window into the crown of the tooth to expose the pulp chamber.
- Tissue Extirpation and Canal Shaping: The endodontist removes the diseased pulp from both the upper chamber and the narrow roots using small, flexible endodontic files.
- Chemical Irrigation: The interior channels are flushed with antibacterial solutions to dissolve organic debris and sterilize the complex root anatomy.
- Canal Obturation: The sterilized, dry canals are tightly packed with gutta-percha cones coated in an endodontic sealer to create a permanent, hermetic barrier against future bacterial penetration.
- Structural Restoration: The access hole is sealed with a temporary filling. Because root-treated teeth become more brittle over time, you will typically return a couple of weeks later for a permanent core buildup and a custom porcelain crown.
Long-Term Outcomes, Success Rates, and Prognosis
When deciding between pulp capping vs root canal, long-term predictability is a major consideration. Both procedures offer good success rates, but their predictability varies based on the tooth’s initial condition and the patient’s age.
Analyzing the Data
- Pulp Capping Longevity: When performed under ideal conditions—such as a clean mechanical exposure in an asymptomatic, young tooth—direct pulp capping using modern MTA can achieve clinical success rates between 90% and 100% after one year (Pinto, 2023). However, when performed on teeth with deep carious decay, the success rate can drop closer to 48% due to pre-existing, deep-seated bacterial infiltration (Sitaru, 2011).
- Root Canal Predictability: Traditional root canal therapy on a vital tooth is highly predictable, maintaining a long-term success rate of 92% to 95% when performed by a skilled clinician (Brodén, 2016; Zhu et al., 2024). It remains a reliable standard for eliminating active infections.
Expected Success Rates Under Ideal Clinical Conditions:
Modern MTA Pulp Cap (Mechanical Exposure): ████████████████████ 90% - 100%
Standard Root Canal Therapy (Vital Tooth): ███████████████████░ 92% - 95%
Carious Exposure Pulp Cap (Deep Decay): ██████████░░░░░░░░░░ 48%
The Impact of Patient Age
Patient age plays a major role in vital pulp therapy outcomes. Younger patients have large pulp chambers with excellent blood flow and a high density of active cells, which gives their teeth a strong natural healing capacity (Sitaru, 2011). As we age, our dental pulps naturally undergo a process called fibrous recession. The pulp chamber shrinks, blood vessels narrow, and the tissue loses some of its regenerative potential, making root canal therapy more likely for older individuals (Scalzilli, 0).
Financial Considerations and Insurance Coverage
The cost differences between these two procedures can impact your out-of-pocket dental expenses.
Cost Breakdown
- Pulp Capping Costs: A pulp cap is an affordable addition to a standard filling. The procedure typically adds $150 to $350 to your treatment cost, making it a very cost-effective way to save a tooth if the clinical conditions are right (Scalzilli, 0).
- Root Canal Treatment Costs: A root canal is a multi-step procedure that requires specialized endodontic instruments. Depending on whether the tooth is a single-rooted anterior or a multi-rooted molar, the procedure alone ranges from $800 to $1,600. When you add the required structural core buildup and a custom protective porcelain crown ($1,000 to $2,000), the total investment can range from $1,800 to $3,600+.
Insurance and Long-Term Value
Most dental insurance plans cover pulp capping under standard restorative provisions, though some view direct caps as part of the overall filling charge. Root canal therapy and subsequent crowns are usually classified as major restorative services, typically covered at 50% to 80% after you meet your annual deductible.
While pulp capping is much less expensive upfront, it carries a higher risk of needing a future root canal if the nerve fails to heal. However, when successful, preserving a vital, hydrated tooth offers excellent long-term biological value.
Conclusion
The choice between pulp capping and a root canal comes down to a balance between conservative preservation and predictable infection control. Pulp capping aims to save the tooth’s living tissue using advanced bioactive materials, while a root canal completely removes infected pulp to provide a long-term solution for advanced decay. Consulting with your dentist and taking timely X-rays will help determine the safest, most effective path for your smile.
Frequently Asked Questions (FAQ)
1. Is a pulp capping procedure painful for the patient?
No. The dentist administers standard local anesthesia to completely numb the target tooth and surrounding gums before beginning any work. You should only feel routine pressure during the procedure. Mild, temporary sensitivity is normal for a few days afterward as the pulp tissue heals.
2. How long must I wait to know if a direct pulp cap has succeeded?
Dentists generally monitor a pulp-capped tooth closely for 6 to 24 months. You will return for routine follow-up visits so your provider can check the tooth’s vitality with thermal tests and take periodic X-rays to ensure a new dentin bridge has formed without any signs of deep infection (Sitaru, 2011).
3. What happens if a pulp cap fails?
If the internal tissue cannot recover, the pulp will gradually become necrotic. Symptoms of failure include a persistent, throbbing ache, prolonged sensitivity to heat, or a localized swelling on your gums. If this occurs, the dentist can perform a standard root canal to clear the infection and save the outer tooth structure.
4. Can every tooth with a deep cavity be treated with an indirect pulp cap?
No. A tooth is only a candidate if the pulp is still fully vital and shows no signs of chronic, irreversible inflammation. If you experience spontaneous, throbbing pain at night or if an X-ray reveals a dark abscess around the root tip, vital pulp capping is no longer an option, and a root canal is required.
References
- Alp, Ş., & Ulusoy, N. (2024). Current Approaches in Pulp Capping: A Review. Cyprus Journal of Medical Sciences, 154-160. https://doi.org/10.4274/cjms.2023.2022-37
- Cited by: 17
- Alshargawi, W., Alaamer, S., Alharabi, E., Alzaid, S., Alghamdi, S., Almarshedy, B., Alhammad, A., ALharbi, N., Alshammari, S., Aldahami, M., & Alhaif, A. (2023). The Influence of Pulp Capping Procedures on the Long-Term Prognosis and Survival of Teeth. JOURNAL OF HEALTHCARE SCIENCES, 03, 241-247. https://doi.org/10.52533/johs.2023.30708
- Cited by: 0
- Brodén, J. (2016). Direct pulp capping procedures versus root canal treatment in young permanent vital teeth with pulp exposure due to caries. A systematic review. the American Journal of Dentistry, 29, 201-207.
- Cited by: 21
- Boutsiouki, C., Frankenberger, R., & Krämer, N. (2018). Relative effectiveness of direct and indirect pulp capping in the primary dentition. European Archives of Paediatric Dentistry, 19, 297-309. https://doi.org/10.1007/s40368-018-0360-x
- Cited by: 47
- Islam, R., Islam, M. R. R., Tanaka, T., Alam, M. K., Ahmed, H. M. A., & Sano, H. (2023). Direct pulp capping procedures – Evidence and practice. Japanese Dental Science Review, 59, 48-61. https://doi.org/10.1016/j.jdsr.2023.02.002
- Cited by: 149
- Pinto, K. P. (2023). Success rate of direct pulp capping on permanent teeth using bioactive materials: a systematic review and meta-analysis of randomized clinical trials. Restorative Dentistry & Endodontics.
- Cited by: 16
- Scalzilli, P. A. (n.d.). Decision-making for dental pulp exposure: a survey in graduate programs at Brazilian universities. Brazilian Oral Research.
- Cited by: 11
- Sitaru, A. (2011). Clinical and Radiographic Evaluation of Direct Pulp Capping Procedures in Permanent Teeth. Acta Medica Marisiensis.
- Cited by: 2
- Zhu, L., Liu, W., Deng, X., Chen, Z., Chen, J., & Qian, W. (2024). Full pulpotomy versus root canal therapy in mature teeth with irreversible pulpitis: a randomized controlled trial. BMC Oral Health, 24. https://doi.org/10.1186/s12903-024-05011-0
- Cited by: 16



