Can You Have Dental Implants With Bone Loss?
If you have been told you need dental implants but also that your jawbone is “too thin” or “too soft,” you might feel like you have hit a dead end. That feeling is completely understandable. Bone loss sounds permanent. It sounds scary. And when you hear that implants need solid bone to hold them in place, you might think the answer is simply no.
But here is the truth that many people do not know.
The short answer is yes, in most cases, you can still have dental implants even if you have bone loss. However, the path to getting them looks different. It takes more planning. It takes more time. And it requires a specialist who knows exactly how to work with compromised bone.
This guide will walk you through everything you need to know. No fluff. No fake promises. Just a realistic, honest look at what is possible, what is not, and how modern dentistry solves the bone problem.
Let us start with the basics.
Understanding Bone Loss: Why It Happens and Why It Matters
Before we talk about solutions, we need to talk about the problem. Bone loss in your jaw does not happen overnight. It happens slowly, often without you noticing until it is advanced.
What is jawbone density?
Think of your jawbone like the foundation of a house. A strong, thick foundation can hold heavy structures. A thin, cracked, or soft foundation cannot. Dental implants are small titanium posts that act like artificial tooth roots. They need that strong foundation to fuse with the bone. This process is called osseointegration.
Without enough bone density or height, the implant cannot stay stable. It might loosen. It might fail. Or it might damage nearby nerves and teeth.
The main causes of bone loss in the jaw
Bone loss does not happen randomly. There are clear reasons why your jawbone might shrink or weaken.
| Cause of Bone Loss | How It Affects the Jaw | How Common It Is |
|---|---|---|
| Tooth extraction without replacement | The bone no longer receives stimulation from chewing, so it resorbs (shrinks) | Extremely common |
| Periodontal (gum) disease | Chronic infection eats away at the bone supporting your teeth | Very common |
| Trauma or injury | A broken jaw or lost tooth from an accident can damage bone structure | Less common |
| Long-term denture wear | Dentures rest on the gums and do not stimulate the bone, leading to slow shrinkage | Very common |
| Osteoporosis | A systemic condition that weakens all bones, including the jaw | Moderately common |
| Infection (abscess) | Deep infection can destroy bone tissue around a tooth root | Common |
Note for readers: The most frequent cause of severe bone loss is simply waiting too long after losing a tooth. The first six to twelve months after an extraction are critical. After that, the bone can shrink up to 25% in the first year alone.
How do you know if you have bone loss?
You cannot always feel it. Many patients are shocked when their dentist shows them an X-ray or a 3D CT scan. The bone that looks full and healthy from the outside can be hollow or thin underneath.
Common signs include:
- Loose dentures that used to fit well
- A sunken or collapsed look to your lower face
- Difficulty chewing on one side
- Gum recession that keeps getting worse
- Teeth shifting or tilting into empty spaces
If you have any of these signs, do not panic. You simply need a proper evaluation.
Can You Really Have Implants With Bone Loss? The Straight Answer
Let us be direct. You can have dental implants with bone loss, but not without addressing the bone loss first or choosing a specific type of implant.
Think of it like this: You cannot build a two-story house on swampy ground. You either drain and reinforce the ground, or you build a different kind of foundation.
The same logic applies here.
Three realistic scenarios for implants with bone loss
Scenario one: Mild bone loss
You have lost a little bit of bone height or width, but there is still enough to support a standard-sized implant. Your dentist might place the implant immediately. No extra procedures needed. This is the easiest case.
Scenario two: Moderate bone loss
You have lost enough bone that a standard implant is risky. However, you are a good candidate for a bone graft or a sinus lift. These procedures rebuild the bone first. Then, after several months of healing, you get the implant.
Scenario three: Severe bone loss
Your jawbone is very thin, short, or soft. A traditional implant is not possible, even with grafting. But you are not out of options. You may be a candidate for zygomatic implants (anchored in the cheekbone) or mini-implants (smaller posts for lower forces).
Important: No ethical dentist will place an implant into insufficient bone just because you ask for it. If someone promises you same-day implants without any imaging or bone assessment, walk away. That is a red flag.
What the research actually says
Clinical studies show that dental implants placed into bone-grafted sites have a success rate of 85% to 95% after five to ten years. That is only slightly lower than implants placed into natural, healthy bone (which is around 95% to 98%).
So yes. Rebuilding bone works. But it adds time. And it adds cost.
Bone Grafting: The Most Common Solution
If your dentist says you have bone loss, the first solution they will probably mention is a bone graft. Let us break down what that actually means.
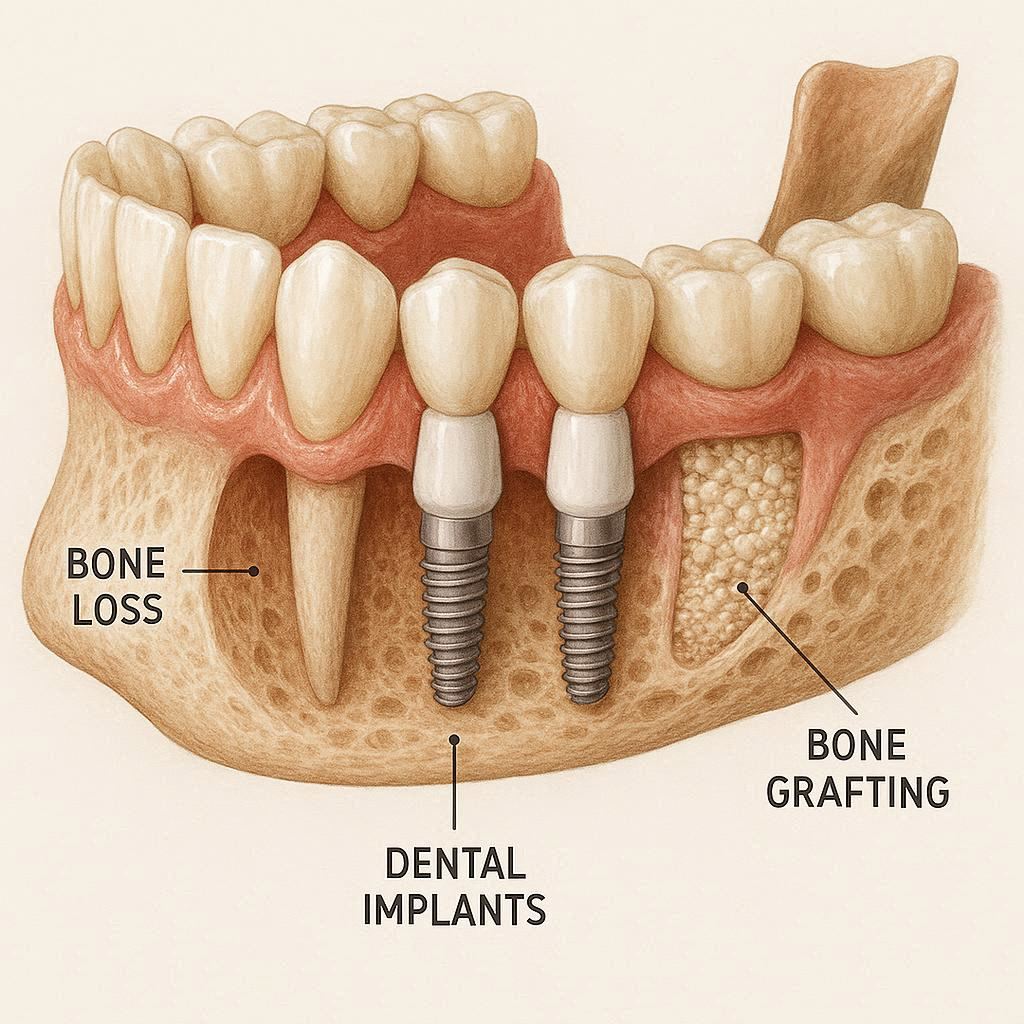
What is a bone graft?
A bone graft is a surgical procedure where your dentist adds bone material to your jaw. This material acts as a scaffold. Your body slowly replaces it with your own natural bone over several months.
Think of it like adding soil to a garden bed before planting seeds. The new soil gives the roots something to grab onto.
Types of bone graft materials
| Type of Graft | Source | Pros | Cons |
|---|---|---|---|
| Autograft | Your own body (often from your chin or hip) | Gold standard; best healing | Second surgery site; more pain |
| Allograft | Donated human bone (processed and sterilized) | No second surgery; widely available | Slightly slower healing |
| Xenograft | Animal bone (usually cow) | Very safe; good structure | Takes longer to remodel |
| Alloplast | Synthetic material (lab-made) | No risk of disease; predictable | Less natural feel |
Most dental offices use allografts or xenografts. You do not need to panic about “cow bone.” These materials are processed to be completely safe and sterile.
What does the procedure look like?
The honest version: It is not fun, but it is manageable.
- Numbing: You get local anesthesia. You are awake but feel no pain.
- Incision: The dentist makes a small cut in your gum to expose the bone.
- Grafting: The bone material is packed into the thin area.
- Protection: A membrane may be placed over it. Then the gum is stitched closed.
- Healing: You wait. Usually four to nine months.
During the healing time, the graft fuses with your existing bone. You wear a temporary tooth or denture if needed.
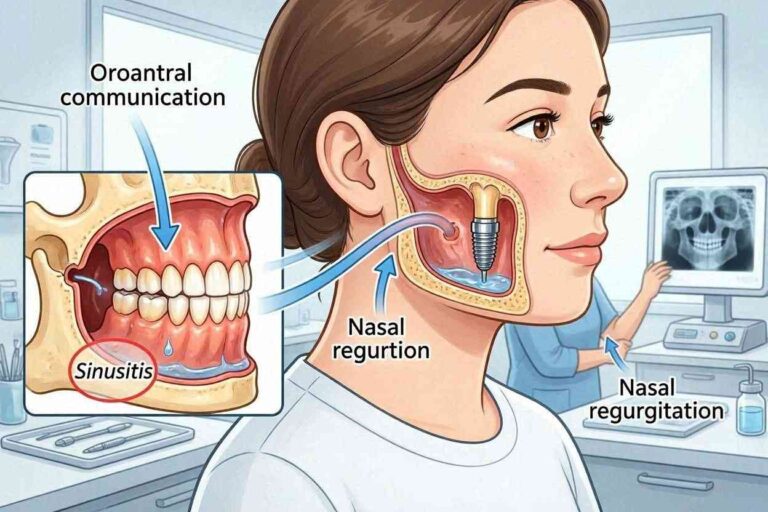
Sinus lifts: A special kind of graft for upper molars
If you are missing upper back teeth (molars or premolars), the maxillary sinus sits right above your jawbone. When bone loss happens, the sinus expands downward. There is no room for an implant.
A sinus lift is a procedure where the dentist gently pushes the sinus membrane up and places bone graft material underneath. It sounds dramatic. In reality, it is a routine procedure done thousands of times every day.
Healing time for a sinus lift is usually six to nine months.
Alternatives to Grafting: When You Cannot or Do Not Want a Graft
Bone grafting is the most common path, but it is not the only path. Some patients cannot have a graft. Others simply do not want to wait that long.
Here are realistic alternatives.
Short implants
Standard implants are usually 10mm to 16mm long. Short implants are 6mm or less. They are designed specifically for jaws with reduced bone height.
Pros:
- No grafting needed in many cases
- Faster treatment (sometimes same-day placement)
- Lower cost than graft + implant
Cons:
- Not suitable for very soft bone
- Higher failure rate than standard implants in some studies (but still over 90% success)
- Not ideal for areas with high chewing forces (like lower molars)
Mini dental implants (MDIs)
Mini implants are about half the width of a standard implant. They look like a small screw with a ball-shaped top. They are often used to secure dentures.
Pros:
- Can be placed in very thin bone (as little as 2mm width)
- Minimally invasive; often no cutting or stitches
- Much lower cost
- Same-day placement and loading
Cons:
- Not as strong as standard implants
- Better for denture stabilization than single crowns
- Shorter lifespan on average (5 to 10 years vs. 20+ years for standard)
Reader note: Mini implants are excellent for lower dentures that click and move. They are less ideal for replacing a single tooth in a high-chewing area.
Zygomatic implants
This is the big gun. Zygomatic implants are extra-long implants (up to 50mm) that anchor not into the jawbone, but into the zygomatic bone — your cheekbone.
Who needs this?
People with severe upper jaw bone loss who have been told “no implants ever.” This includes patients with:
- Long-term denture wear with severe resorption
- Failed bone grafts
- Bone loss from tumors or trauma
- Cleft palate defects
Pros:
- No bone grafting required
- Immediate function possible
- Lifespan similar to standard implants
Cons:
- Very complex surgery; requires a specialist (oral surgeon or prosthodontist)
- Expensive ($20,000 to $40,000 per arch)
- Longer recovery
- Not available everywhere
Pterygoid implants
Less common but worth mentioning. Pterygoid implants anchor into the pterygoid plate, a bone structure at the very back of the upper jaw. They bypass the sinus and the thin alveolar bone entirely.
These are usually combined with zygomatic implants in full-arch reconstructions.
The Step-by-Step Process for Implants With Bone Loss
If you decide to move forward, here is what your journey will look like from start to finish. This timeline assumes you need a bone graft.
Phase one: Diagnosis and planning (1 to 2 visits)
Your dentist will not guess. They will measure.
- 3D CBCT scan: This is a special X-ray that creates a 3D model of your jaw. It shows bone height, width, density, and the location of nerves and sinuses.
- Treatment planning software: The dentist virtually places the implant in the scan to see if it fits.
- Medical review: Conditions like uncontrolled diabetes, heavy smoking, or bisphosphonate use (bone medications) can affect success.
Quote from a prosthodontist: *”I never promise an implant until I see the CBCT scan. Patients are often surprised that what looks fine on a normal X-ray is actually too thin in 3D.”*
Phase two: Bone grafting (one surgery, then 4 to 9 months of healing)
The graft is placed. You go home with pain medication and antibiotics. Most people say the pain is similar to a tooth extraction — manageable with over-the-counter meds after the first two days.
During healing, the graft material turns into living bone. You cannot speed this up. Your body needs time.
Phase three: Implant placement (one surgery, then 3 to 6 months of healing)
Once the graft is solid, the dentist places the titanium implant. This surgery is usually quicker than the graft. The implant is buried under the gum or has a healing cap exposed.
Again, you wait. The bone grows tightly around the implant surface. This is osseointegration.
Phase four: Abutment and crown (2 to 3 visits over 1 month)
A small connector (abutment) is attached to the implant. Then a custom-made crown is cemented or screwed on.
At this point — often 12 to 18 months after you started — you have a finished tooth.
Factors That Affect Your Success Rate
Not everyone with bone loss has the same chance of success. Be honest with yourself about these factors.
Smoking
This is the biggest modifiable risk factor. Smoking restricts blood flow to the gums and bone. It dramatically slows healing.
The numbers:
- Non-smokers: 95%+ implant success
- Light smokers (less than 10/day): 85-90% success
- Heavy smokers (more than 20/day): 70-80% success
If you smoke, your dentist will likely ask you to quit for at least two weeks before surgery and throughout the healing period. Some will refuse surgery unless you commit to quitting.
Diabetes
Controlled diabetes is fine. Uncontrolled diabetes (HbA1c above 8%) is a real problem. High blood sugar impairs healing and increases infection risk.
What you need: A recent HbA1c test showing stable control. Coordinate with your primary care doctor.
Medications
Bisphosphonates (Fosamax, Actonel, Boniva, Reclast) used for osteoporosis are a concern. They can cause a rare but serious condition called medication-related osteonecrosis of the jaw (MRONJ). This is where the jawbone dies after a dental surgery.
If you have taken oral bisphosphonates for less than three years, the risk is low but not zero. If you have taken them for more than four years or had IV bisphosphonates (for cancer), implants may be too risky.
Always bring a complete medication list to your consultation.
Bruxism (teeth grinding)
If you grind your teeth at night, you put extreme forces on implants. Implants do not have the shock-absorbing ligament that natural teeth have. They can crack or loosen.
Solution: A custom nightguard worn every night. No exceptions.
Costs: What You Will Actually Pay
Let us talk money. This is where many people get sticker shock.
Bone grafting and implants are not cheap. But the range is wide depending on where you live and what you need.
Average costs in the United States (without insurance)
| Procedure | Typical Cost Range |
|---|---|
| Single standard implant (implant + abutment + crown) | $3,000 – $6,000 |
| Bone graft (small, one site) | $500 – $1,500 |
| Bone graft (large, multiple sites) | $2,000 – $5,000 |
| Sinus lift | $1,500 – $3,000 |
| Mini implant (per implant, including crown) | $1,000 – $2,500 |
| Zygomatic implant (per arch, 4 implants) | $20,000 – $40,000 |
| Full-arch fixed bridge (All-on-4 with grafting) | $20,000 – $35,000 per arch |
Does insurance cover any of this?
Traditional dental insurance often excludes implants. But it may cover:
- Bone grafting if deemed “medically necessary”
- Extractions and temporary dentures
- Portions of the crown
Some medical insurance plans cover implants if tooth loss was due to trauma, tumor removal, or a congenital condition. Always ask.
Financing options
Most dental offices offer third-party financing:
- CareCredit: No-interest if paid in full within 6-12 months
- LendingClub: Fixed monthly payments
- In-house payment plans: Rare but ask
Do not let cost alone stop you from a consultation. Many offices offer free or low-cost CBCT scans for new patients.
When the Answer Is Honestly “No”
I promised you an honest guide. So here is the hard truth.
There are situations where even the most advanced techniques cannot safely place an implant.
Absolute contraindications (no implants, ever)
- Active, untreated cancer (especially head and neck radiation)
- Severe untreated bleeding disorders
- Active IV bisphosphonate use (high risk of osteonecrosis)
- Current IV drug use (high infection and failure rate)
Relative contraindications (possible but very high risk)
- Severe uncontrolled diabetes (HbA1c >9%)
- Heavy smoking (more than two packs per day)
- Severe immunosuppression (organ transplant, uncontrolled HIV)
- Extreme bone loss with failed prior grafts
In these cases, your dentist will likely recommend alternatives like:
- High-quality dentures with adhesive
- Implant-supported dentures using mini implants (if bone is borderline)
- Partial dentures for single missing teeth
Note: Getting a “no” from one dentist does not mean every dentist will say no. Specialist opinions vary. But if two oral surgeons tell you no, listen to them.
How to Prepare for Your Consultation
Walk into your appointment ready. Here is what you need to bring and ask.
What to bring
- Recent X-rays (if any)
- List of all medications and supplements
- Medical history summary (especially diabetes, osteoporosis, cancer)
- Your dental insurance card
- A notepad or phone for notes
Questions to ask your dentist
- “Based on my CBCT scan, how much bone do I actually have in millimeters?”
- “Are you recommending a graft, a short implant, or another option? Why?”
- “What is your personal success rate with patients like me?”
- “How many of these procedures have you done?”
- “What happens if the graft fails? Do I get a refund or a retry?”
- “Can I see before-and-after photos of similar cases?”
Red flags to watch for
- A dentist who places implants without a CBCT scan
- Promises of “same-day implants for everyone”
- No discussion of your medical history
- Vague answers about costs
- Pressure to decide immediately
A good specialist will be happy to answer all your questions. If they seem annoyed, find another provider.
Living With Implants After Bone Loss
Once your implants are in and healed, your life changes. But you also have new responsibilities.
How to care for your grafted-bone implants
- Brush and floss normally (use superfloss or water flossers around implants)
- Avoid hard foods (ice, hard candy, bones) for the first year
- Wear a nightguard if you grind
- Visit your dentist every six months for professional cleaning and X-rays
What is normal and what is not
Normal:
- Slight gum sensitivity for the first week after crown placement
- A small amount of gum recession over many years
- The crown may need tightening every 5-10 years
Not normal (call your dentist):
- The implant feels loose at any time
- Persistent pain or swelling months after healing
- Bleeding around the implant when brushing
- The gum around the implant turns dark red or purple
Lifespan expectations
| Type | Average Lifespan | Can it be replaced? |
|---|---|---|
| Standard implant with graft | 20+ years (often lifetime) | Yes, but complex |
| Short implant | 15-20 years | Yes |
| Mini implant | 5-10 years | Yes, easier than standard |
| Zygomatic implant | 20+ years | Very complex |
Conclusion (Summarized in Three Lines)
You can have dental implants with bone loss, but you will likely need a bone graft, a sinus lift, or a specialized implant like a short or zygomatic implant. The process takes longer (often 12 to 18 months) and costs more, but success rates are excellent — 85% to 95% — when performed by an experienced specialist. Be honest about your smoking, diabetes, and medication use, because those factors matter more than the bone loss itself.
Frequently Asked Questions (FAQ)
1. Can I get dental implants years after bone loss has occurred?
Yes. Even if you lost teeth ten or twenty years ago, bone grafting can rebuild what is missing. It just takes longer and may require more extensive grafting.
2. How much bone is needed for a dental implant?
As a general rule: 10mm of height and 6mm of width for a standard implant. But short implants need only 5-6mm of height, and mini implants need as little as 2mm of width.
3. Is bone grafting painful?
You will be numb during the procedure. Afterward, most people describe it as moderate discomfort for 2-3 days, similar to a tooth extraction. Over-the-counter pain relievers usually work.
4. How long do I have to wait between bone grafting and implant placement?
Typically 4 to 9 months. The graft needs time to turn into living bone. Trying to place the implant too early leads to failure.
5. Can bone loss continue after implants are placed?
Yes, if you have active gum disease or bruxism (grinding). Otherwise, the implant itself stops bone loss in that specific area because it provides chewing stimulation.
6. Are mini implants a good long-term solution?
For securing dentures, yes. For replacing a single molar that chews hard food, no. Match the implant type to the job.
7. What is the success rate of dental implants with bone grafting?
Around 85% to 95% after 5-10 years. The success rate depends more on your health habits (smoking, diabetes control) than on the graft itself.
8. Can I get a full set of implants if I have severe bone loss?
Yes. Many patients with severe bone loss receive full-arch fixed bridges using zygomatic implants or multiple standard implants with extensive grafting. The All-on-4 technique is one popular option.
9. Will my insurance cover bone grafting for implants?
Sometimes. If the bone loss is from a traumatic injury or tumor removal, medical insurance may help. For routine tooth loss, dental insurance rarely covers grafting or implants.
10. What happens if an implant with bone grafting fails?
The implant is removed. The area is allowed to heal. A second graft may be attempted, or you may consider mini implants or a denture. Do not panic — failure is not the end of the road.
Additional Resource
For a deeper dive into the clinical studies behind bone grafting and implant success rates, visit the American Academy of Implant Dentistry (AAID) patient education library:
👉 www.aaid.com/patient-resources