Dental Implants Periodontist: Why Gum Health Is the Real Foundation of Your New Smile
When you lose a tooth, it feels like a small crisis. You worry about your smile, your ability to chew, and even how you speak. In that moment of worry, most people start searching for a solution. They hear about dental implants. They hear they are the “gold standard.” But then comes the big question: Who is actually qualified to put that implant into your jaw?
You might think any dentist can do it. Technically, many can. But there is one specialist who studies the very ground where that implant must live: the periodontist.
Think of a dental implant like building a house. You can buy the most expensive windows, doors, and roof tiles. You can hire an artist to paint the walls. But if you build that house on shifting sand or muddy water, it will fall apart within a year. The periodontist is the geologist and the foundation builder combined. They don’t just place the tooth; they make sure the bone and gums are healthy enough to support it for thirty years.
This guide is not just a collection of facts. It is a realistic, honest walk through the world of dental implants from a periodontist’s perspective. We will look at costs, pain levels, recovery, and why choosing the right specialist matters more than the brand of the implant.
By the end, you will feel confident, informed, and ready to make a decision that affects your health for a lifetime.

1. Understanding the Specialist: What Exactly Is a Periodontist?
Let’s clear up a common confusion right away. A general dentist is like your family doctor. They check your teeth, fill cavities, and handle routine cleanings. They are essential. But when something goes wrong with the “ground” your teeth sit in—the gums and jawbone—you need a specialist.
A periodontist is a dentist who has completed three years of extra rigorous training after dental school. During those three years, they focus exclusively on:
- Inflammatory diseases: Gum disease (gingivitis and periodontitis).
- Soft tissue: Your gums.
- Hard tissue: The alveolar bone (the bone that holds your teeth).
The Surgical Mindset
Because they deal with infections and bone loss every day, periodontists are experts in surgery. They are not just drilling a hole and screwing in a post. They are evaluating blood supply, bone density, and tissue thickness.
“A general dentist fixes teeth. A periodontist saves the foundation that holds the teeth in place.” — Dr. Elena Vasquez, Board Certified Periodontist
When a periodontist places a dental implant, they are not “borrowing” skills from another area of dentistry. They are using their primary specialty.
Why does this matter for implants?
Implants fail for two reasons: infection (peri-implantitis) or lack of bone support. Both of these live in the periodontist’s wheelhouse. If you have ever had bleeding gums, receding gums, or a loose tooth in the past, your risk for implant failure is higher. A periodontist knows how to mitigate that risk before they even touch the implant.
2. The Anatomy of an Implant: A Simple Breakdown
Before we go further, let’s look at the hardware itself. Understanding the parts helps you understand the process.
| Component | What it is | Role | Material |
|---|---|---|---|
| The Fixture (Post) | The screw inserted into the jawbone. | Acts as the artificial tooth root. Provides stability. | Medical-grade Titanium or Zirconia (ceramic). |
| The Abutment | A connector piece. | Joins the post to the crown. Sits at or above the gum line. | Titanium, Gold, or Zirconia. |
| The Prosthesis (Crown) | The visible “tooth.” | Restores chewing function and aesthetics. | Porcelain fused to metal, or solid ceramic. |
When these three parts work in harmony, you get a tooth that feels and acts exactly like a natural one. However, the periodontist’s main focus is on the Fixture. If that post does not fuse with your bone (a process called osseointegration), the other two parts are worthless.
A Note on Materials
- Titanium: The gold standard for 50+ years. Highly biocompatible. Rare allergies.
- Zirconia: Metal-free. White in color. Great for patients with metal sensitivities. Newer technology.
Your periodontist will help you choose based on your medical history and aesthetics. There is no “best” material for everyone. There is only the best material for you.
3. The Comprehensive Consultation: What to Expect
You book an appointment with a periodontist. You are nervous. You don’t know what they are going to find. A professional periodontist will never rush to surgery. In fact, a good one will try to talk you out of an implant if your mouth isn’t ready.
Here is what happens during that first visit:
Step 1: The Probe (No Pain, Just Data)
The doctor will take a small measuring instrument (a periodontal probe) and gently measure the pockets between your remaining teeth and gums. Healthy pockets are 1-3 mm deep. Pockets over 4 mm indicate inflammation.
Step 2: The CBCT Scan (The X-ray that changes everything)
You stand while a machine rotates around your head. This is not a normal dental x-ray. This is a Cone Beam CT Scan. It gives the periodontist a 3D map of your skull.
- They will look for: Bone height, bone width, nerve location, and sinus position.
- Honest reality: They might look at the scan and say, “You have no bone left here.”
Step 3: The Medical History Review
Periodontists are medical doctors of the mouth. They will ask about:
- Diabetes (uncontrolled sugar kills implants).
- Smoking (constricts blood vessels in the gums).
- Osteoporosis medications (bisphosphonates can cause bone death).
- Heart conditions (need antibiotics pre-surgery).
Step 4: The “Yes or No” Conversation
A responsible periodontist will tell you the truth. They might say:
- “Yes, we can do this tomorrow.”
- “Yes, but you need gum disease treatment first.”
- “No, we need to build bone before we even think about an implant.”
Important Note: If a specialist tells you “no” or “not yet,” thank them. They just saved you $5,000 and years of pain.
4. Preparing the Soil: Bone Grafting and Ridge Preservation
Here is the most skipped step by general dentists, and the most performed step by periodontists: bone grafting.
When you lose a tooth, the bone that surrounded that tooth starts to melt away. It is a biological fact. Bone needs stimulation from a root to exist. Without the root, the body says, “We don’t need this real estate,” and reabsorbs the minerals.
The 60-Day Rule
Within 60 days of losing a tooth, you have lost up to 40% of the bone width in that spot. You can’t see it, but it is happening under your gums.
Types of Grafts a Periodontist Uses
| Graft Type | Source | Pros | Cons |
|---|---|---|---|
| Autograft | Your own bone (usually from chin or hip). | Gold standard. Living cells. Best results. | Requires second surgical site. More pain. |
| Allograft | Donor human bone (sterilized). | No second surgery. Safe. Widely available. | Slower integration than autograft. |
| Xenograft | Cow or pig bone. | Unlimited supply. Great for volume. | Takes longer to turn into human bone. |
| Alloplast | Synthetic lab-made bone. | No disease risk. Predictable. | Lacks natural growth proteins. |
The Realistic Timeline:
If you need a bone graft, do not expect an implant tomorrow.
- Extraction + Graft: Day 1.
- Healing: 4 to 9 months. (Yes, months. Bone grows slowly.)
- Implant placement: After bone is hard.
- Osseointegration: Another 3 to 6 months.
- Final tooth: 6 to 12 months after extraction.
Waiting is frustrating. But rushing leads to an implant that wobbles in soft bone. A periodontist will always prioritize biology over convenience.
5. The Surgical Procedure: A Step-by-Step Walkthrough
You have healthy gums. You have dense bone. It is surgery day. Let’s walk through the room so you know exactly what happens. No surprises.
Anesthesia (The Easy Part)
You will be numb. Periodontists use local anesthetic (lidocaine) with epinephrine. The epinephrine is key—it shrinks blood vessels to reduce bleeding and keep the area clear. If you are anxious, they offer sedation (pill or IV). You will be awake but very relaxed, or asleep entirely.
Step 1: The Incision (Precision cutting)
Using a tiny scalpel, the periodontist makes a precise cut in your gum. They lift a flap of gum tissue back to expose the bare jawbone. You feel pressure, but zero pain.
Step 2: The Pilot Hole (The critical moment)
Using the CT scan like a GPS, the doctor drills a very small pilot hole. This must be in the exact center of the bone, at the perfect angle.
- Too deep: You hit the nerve (lower jaw) or sinus (upper jaw).
- Too shallow: The crown will be too long.
- Too tilted: The tooth will look crooked.
Periodontists often use surgical guides—3D printed stents that fit over your teeth to guide the drill perfectly.
Step 3: Sequential Drilling
The doctor gradually uses bigger and bigger drills to widen the hole. They constantly irrigate (spray) the area with cold saline to prevent heat. Heat kills bone. If the bone gets hot (over 47°C/117°F), the cells die and the implant fails. This is a common error by inexperienced hands.
Step 4: Placing the Implant
The titanium post is screwed into the prepared hole. It requires a specific amount of force called “insertion torque.” Too little, it wobbles. Too much, it cracks the bone. A periodontist has the tactile feel for this pressure.
Step 5: The Healing Cap
A small screw is placed on top of the implant to keep the gum tissue from growing over the hole. Then, the gum is sutured (stitched) closed over or around the implant.
Duration: Single implant usually takes 45 to 60 minutes.
Immediate Post-Op
You will bite on a gauze pad for 30 minutes. Your periodontist will send you home with:
- Antibiotics (to prevent infection).
- Prescription painkillers (or strong ibuprofen).
- A special mouthwash (chlorhexidine).
- An ice pack (20 minutes on, 20 minutes off).
6. The Reality of Recovery: Week by Week
Let’s be honest. The internet is full of horror stories and miracle stories. The truth is in the middle. Here is a realistic timeline of what actually happens after implant surgery.
Days 1-3: The Swelling Phase
- Pain level: 5/10. You will feel throbbing.
- What you see: Puffy cheek (like a hamster), minor bruising.
- Diet: Only cold soft food. Smoothies (no straw!), yogurt, apple sauce, cold soup.
- Activity: Rest. Head elevated on two pillows to reduce swelling.
- No-nos: No spitting, no swishing, no drinking alcohol, no smoking.
Days 4-7: The Healing Phase
- Pain level: 2/10. You likely stop painkillers.
- What you see: Swelling goes down. Stitches might feel “tight.”
- Diet: Warm soft food. Mashed potatoes, scrambled eggs, oatmeal.
- Activity: Light walking is fine. No heavy lifting (blood pressure pushes blood into the wound).
Days 7-14: The Suture Removal
- Pain level: 0-1/10. Removal feels like a tiny tickle.
- What happens: The doctor checks for signs of infection (redness, pus, bad taste).
- Diet: Soft foods but you can start chewing on the opposite side.
- Hygiene: You can gently brush near the site with a child’s toothbrush.
Week 3-6: The Silent Integration
- Sensation: It feels “normal” but weird. There is a metal cap there, but no tooth.
- Caution: You might think you are healed. You are not. The bone is fusing slowly.
- Warning sign: If you feel the implant move when you push it with your tongue, call immediately (this is rare but emergent).
“Patients often say the first three days are annoying, not painful. The hardest part is the boredom of soft food, not the surgery itself.” — Patient Survey, American Academy of Periodontology
7. Two-Stage vs. Immediate Loading: Which Is Right for You?
Not all implant surgeries look the same. Periodontists use different protocols depending on your situation. Let’s compare them.
| Feature | Two-Stage (Traditional) | Immediate Loading (Same Day) |
|---|---|---|
| Process | Place implant. Bury it under gum. Wait 4-6 months. Uncover. Add crown. | Place implant. Attach temporary crown the same day. |
| Pros | Very low failure rate. Allows bone to heal without chewing pressure. | You leave with a tooth. No flipper. Better aesthetics immediately. |
| Cons | You wear a temporary partial denture (flipper) for months. | High skill required. Higher risk if bone is soft. |
| Best for | Single molars, smokers, patients with bone grafts. | Front teeth (low chewing force), dense bone, non-smokers. |
| Failure risk | 2-3% | 5-10% |
The unvarnished truth: Many general dentists offer “Teeth in a Day” because it sells. Periodontists offer “Teeth in a Day” only when the math works. If your bone is marginal, a responsible periodontist will insist on the two-stage protocol. Do not let marketing pressure you into a fast solution if your body isn’t ready.
8. Cost Breakdown: What Are You Actually Paying For?
Let’s talk money. Dental implants are expensive. But understanding why helps you accept the price. You are not paying for the screw (which costs the doctor maybe $300). You are paying for the 12+ years of education and the $300,000 CT scanner.
Average Costs in the USA (Without Insurance)
| Service | Provider | Cost Range |
|---|---|---|
| Consultation + CBCT Scan | Periodontist | $350 – $500 |
| Extraction of failed tooth | Periodontist | $200 – $400 |
| Bone graft (if needed) | Periodontist | $600 – $1,200 per site |
| Implant fixture placement | Periodontist | $1,800 – $3,000 |
| Abutment | General Dentist (or Pro) | $300 – $600 |
| Crown (the tooth part) | General Dentist | $1,500 – $3,000 |
| Total Single Tooth (No graft) | Combined | $3,800 – $6,500 |
| Total Single Tooth (With graft) | Combined | $4,500 – $8,000 |
Hidden Costs You Must Ask About
- The Temporary: Will they give you a “flipper” (plastic fake tooth) to wear during healing? That is $200-$500 extra.
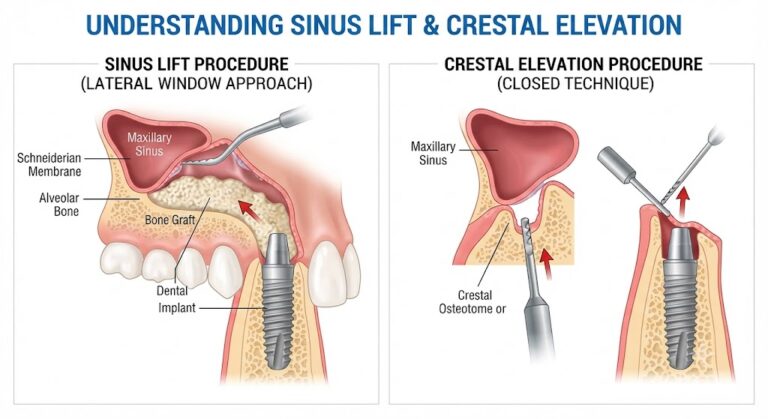
- The Sinus Lift: If you are missing an upper back tooth, the sinus cavity may have dropped down. Lifting the sinus and grafting it is an extra $1,500-$2,500.
- IV Sedation: If you want to sleep through it, add $400-$800 per hour.
Does Insurance Help?
Medical insurance usually says no (they call it “dental”). Dental insurance usually caps at $1,500-$2,000 per year. A single implant blows through that cap. However, if the tooth was knocked out in an accident, your medical insurance might cover the surgical placement. Always fight this battle with your periodontist’s billing coordinator.
9. The Silent Killer: Peri-Implantitis
You got the implant. You love it. You forget about it. That is the danger.
Natural teeth have a biological “seal” called the junctional epithelium. Implants have a weaker seal. Bacteria love this.
Peri-implantitis is gum disease around an implant. It starts with bleeding when you brush. Then the gums swell. Then the bone around the implant dissolves.
- Stage 1 (Mucositis): Gums red, but no bone loss. Reversible.
- Stage 2 (Peri-implantitis): Bone loss. Not reversible.
Why a Periodontist is Your Long-Term Partner
When you see a general dentist for a cleaning, they will polish the crown. A periodontist, however, uses special plastic or titanium instruments to clean the implant. Metal scrapers (used on natural teeth) will scratch the surface of your implant. Bacteria love scratches.
The Maintenance Schedule:
- Every 3 months if you had gum disease before.
- Every 6 months if you have healthy gums.
- Never miss a year. An untreated peri-implantitis usually ends with the implant spinning loose. You cannot save it then.
10. Full Mouth Reconstruction: All-on-4 and All-on-6
What if you are missing all your teeth? Dentures? A periodontist offers a better life: fixed implants that snap into a bridge.
The Concept
Instead of placing 14 implants (one per tooth), the periodontist places 4 or 6 strategic implants. They place them at angles to use the densest bone available. Then they screw a fixed bridge (a full arch of teeth) onto those implants.
The All-on-4 Protocol
| Aspect | Details |
|---|---|
| Number of Implants | 4 per jaw (upper or lower). |
| Anesthesia | IV sedation (you are asleep). |
| Surgery Time | 2-3 hours per jaw. |
| Recovery | Soft food diet for 3 months. |
| Final Bridge | Acrylic (temp) day one. Porcelain (final) after 6 months. |
| Cost per arch | $15,000 – $30,000. |
| Lifespan | 15-20 years with proper cleaning (special floss threaders). |
Is this better than dentures?
- Dentures: Slip, click, cover your palate (affects taste). Pressure on gums causes bone loss. Face collapses over time.
- All-on-4: Fixed. You don’t remove it. Feels like teeth. Preserves bone because the implants stimulate it.
The downside: If one implant fails in an All-on-4 setup, the whole bridge often has to be remade. That is why you use a periodontist, not a discount chain.
11. Risk Factors: Who Should Not Get Implants?
A good periodontist knows when to say “no.” Let’s be realistic about who is a poor candidate.
Absolute Contraindications (Do not do it)
- Untreated cancer in the jaw/head/neck.
- Active, uncontrolled diabetes (HbA1c > 8.0). Healing is impossible.
- Severe bleeding disorders (Hemophilia).
- Active IV bisphosphonates (bone hardening drugs for osteoporosis). These cause osteonecrosis—jawbone death.
Relative Contraindications (Maybe, with extra care)
- Smoking: Smokers have a 15-20% failure rate vs. 2-3% for non-smokers. If you smoke, you must quit for 2 weeks before and 2 months after surgery.
- Bruxism (Clenching/Grinding): You will break the crown or the screw. You need a night guard before the implant is placed.
- Heavy drinkers: Alcohol thins blood and interferes with bone healing.
Age is not a barrier
80-year-olds get implants successfully all the time. As long as the bone is healthy and the patient is healthy, age is irrelevant.
12. Implants vs. Other Options: A Comparative Table
You have choices. Here is the honest comparison.
| Feature | Dental Implant | Fixed Bridge | Removable Partial Denture |
|---|---|---|---|
| Longevity | 20+ years (often life) | 7-15 years | 3-5 years |
| Cost upfront | High ($4k-$8k) | Medium ($2k-$4k) | Low ($500-$1.5k) |
| Damage to adjacent teeth | None. (Doesn’t touch neighbors). | High. (Shaves down healthy teeth). | Medium. (Clasps wear enamel). |
| Bone preservation | Yes. (Stimulates bone). | No. (Bone under bridge melts). | No. (Bone melts). |
| Cleaning | Brush and floss normally. | Requires floss threaders. | Remove, brush, soak. |
| Comfort | Feels like a real tooth. | Good, but food gets stuck under it. | Poor. Moves while eating. |
The Verdict: A bridge destroys two good teeth to replace one bad one. An implant replaces the bad one and leaves the neighbors alone. If you can afford it and have the bone, the implant is the ethical choice.
13. How to Choose the Right Periodontist (Checklist)
You cannot just pick a name off Google. You need to vet them.
The Interview Questions
Call the office or sit in the chair and ask these five questions:
- “How many implants do you place per month?” (Answer should be >15. You want volume).
- “What is your failure rate?” (Honest answer: 2-3% for single teeth. If they say 0%, they are lying).
- “Do you use a CT scan on every patient?” (Answer must be YES. If they guess the bone, walk out).
- “Who restores the crown?” (Ideally, your general dentist does the crown. The periodontist does the surgery. This split is best practice).
- “What do you do for peri-implantitis?” (Look for answer: Laser therapy, open flap debridement, or referral).
Red Flags
- Price too good: “$999 Implants!” Those are usually not including the crown, or they use cheap Chinese parts.
- No pre-surgical consult: They want to cut on Day 1. Run.
- No post-op follow-up: A periodontist should see you at 2 weeks, 3 months, and 1 year.
14. Pain Management and Anxiety
Fear of pain stops 40% of people from getting implants. Let’s kill that fear with facts.
During Surgery
You won’t feel the cut. You won’t feel the drill. You will feel vibration. It feels weird, like a deep tickle in your skull. It is not painful.
After Surgery (The Honest Truth)
The worst pain is when the local anesthetic wears off 3 hours later.
- Pain scale: 6/10 for 4 hours.
- Solution: Take the first ibuprofen before the numbness wears off. Do not wait for the pain to start.
- Ice is your friend: 20 minutes on, 20 off for the first 6 hours reduces pain by 50%.
The Secret Weapon: Bromelain
Periodontists often recommend bromelain (an enzyme in pineapples) or Arnica Montana. These are natural supplements that dramatically reduce bruising and swelling. Ask your doctor about them.
“Most of my patients tell me the wisdom tooth extraction they had at 18 was worse than this implant. Implants are precise, not violent.” — Dr. Marcus Thorne, DDS, MS
Important Notes for Readers
📌 Bone grafts take time. Do not let anyone rush you into an implant 8 weeks after an extraction if you had an infection. Patience pays in titanium.
📌 Blood flow is healing. If you have high blood pressure or use vasoconstrictors (like some migraine meds), tell your periodontist. They need to adjust the anesthesia.
📌 You do not need to remove the implant for cleaning. Ever. If a dentist tells you to take it out, it is not an implant; it is a denture.
📌 Metal allergies are real but rare. 0.6% of the population reacts to titanium. A zirconia implant is your solution.
📌 Your general dentist is your partner. The periodontist does the surgery. Your regular dentist should make the crown and do the annual checks. You need both.
Conclusion (Three Lines)
Choosing a dental implants periodontist ensures that your new teeth are built on a foundation of healthy bone and gum tissue, drastically reducing the risk of failure. While the process requires patience—sometimes months of healing before the final tooth appears—the result is a permanent, natural-feeling solution that preserves your facial structure. Remember, you are not paying for a metal screw; you are paying for surgical precision and long-term biological success.
Frequently Asked Questions (FAQ)
Q1: Is a periodontist better than an oral surgeon for implants?
A: Both are specialists. Oral surgeons focus on extractions and jaw pathology. Periodontists focus on bone health and gum disease. For a standard implant, a periodontist is excellent. For impacted teeth near a nerve, an oral surgeon might be better. Ask your dentist for a referral based on your specific case.
Q2: How long does a dental implant last?
A: With good hygiene and regular periodontist checkups, 20 years to a lifetime. The crown (tooth part) may wear out after 15 years and need replacement, but the titanium post usually stays forever.
Q3: Can I get an implant if I have receding gums?
A: Yes, but you may need a gum graft first. The periodontist will take tissue from the roof of your mouth to thicken the gum around the implant site. Thin gums around an implant look black and metallic.
Q4: Does getting a dental implant hurt?
A: The procedure itself does not hurt (you are numb). The 3-5 days after surgery involve manageable soreness, similar to a deep bruise. Most patients stop all pain medication by day 4.
Q5: What happens if the implant fails?
A: The periodontist removes it (fairly easy, done in 10 minutes). You let the bone heal for 3 months. Then you try again, often with a larger diameter implant or a bone graft. Failure is not the end; it is a restart.
Q6: Can I smoke with an implant?
A: We strongly advise against it. Smoking cuts blood flow by 50%. Smokers are 3x more likely to lose the implant within 5 years. If you cannot quit, consider a traditional bridge instead.
Q7: Are implants covered by Medicare or Medicaid?
A: Generally, no. Original Medicare does not cover dental implants. Some Medicare Advantage plans (Part C) offer limited dental benefits. Medicaid coverage varies by state but is usually only for children or emergency extractions.
Q8: Do implants feel like real teeth?
A: Yes, remarkably so. The only difference is you don’t feel “hot” or “cold” in the implant because it has no nerve. Chewing pressure feels identical to natural teeth because the bone receptors still work.
Additional Resource
For a verified list of board-certified periodontists in your area and to read patient-reviewed outcome data, visit the American Academy of Periodontology official patient resource page.
🔗 Link: https://www.perio.org/for-patients/
(Note: This is the official governing body for periodontists in the USA. They offer a “Find a Periodontist” tool and downloadable guides on implant maintenance.)
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a licensed periodontist or dental professional for diagnosis and treatment options specific to your oral health condition. Individual results vary based on bone density, health history, and compliance with post-operative care.