Dental Implant Candidacy: A Complete, Honest Guide to Knowing If Implants Are Right for You
You have a missing tooth. Or maybe several. You have heard that dental implants are the “gold standard.” They look natural. They feel strong. They can last a lifetime.
But here is the real question that stops most people: Am I a candidate for dental implants?
You might worry that you are too old. Or that your bone is gone. Or that a health condition will get in the way. These are normal concerns. And the good news is that modern dentistry has changed the rules.
This guide walks you through every single factor that matters. No confusing medical jargon. No unrealistic promises. Just a clear, friendly map to help you understand where you stand.
Let us start with the most common question of all.

What Does “Dental Implant Candidacy” Really Mean?
Being a candidate does not mean you are perfect. It means that a dentist looks at your mouth and your health and decides that an implant has a high chance of success.
Success for a dental implant is usually defined as:
- The implant fuses with your jawbone (osseointegration)
- No pain or infection after healing
- The implant supports a crown, bridge, or denture for years
Candidacy lives on a spectrum. Some people are ideal candidates. Others are conditional candidates—meaning they need a little extra work first. A small number of people are not candidates at all, but that group is smaller than you think.
Important note: Almost 70% of adults aged 35 to 44 have lost at least one permanent tooth. Yet less than 10% of those people currently have implants. Candidacy is often broader than people assume.
The Four Pillars of Dental Implant Candidacy
Every dentist evaluates four main areas. Think of these as four legs on a chair. If one leg is weak, the chair can still work—but you need to reinforce it.
| Pillar | What It Means | Common Issues |
|---|---|---|
| Bone health | Enough jawbone density to hold the implant | Bone loss from missing teeth or gum disease |
| Gum health | No active periodontal disease | Bleeding gums, pockets, infection |
| Overall health | Body can heal and integrate the implant | Diabetes, autoimmune issues, smoking |
| Commitment | Willing to follow aftercare instructions | Missed appointments, poor hygiene |
Let us explore each pillar in detail.
1. Bone Density and Volume: The Foundation
Your jawbone is like soil. A fence post needs firm soil to stand upright. An implant needs dense, thick bone to fuse with.
When you lose a tooth, the bone that used to hold that tooth starts to melt away. This is called resorption. In the first year after losing a tooth, you can lose 25% of the bone width. Over time, that number climbs.
How Do Dentists Measure Bone?
They do not guess. They use imaging:
- Panoramic X-ray – gives a 2D view. Good for a first look.
- CBCT scan (Cone Beam CT) – a 3D scan. This is the gold standard. It shows height, width, and density of your bone.
A CBCT scan takes about 20 seconds. It is painless. And it gives your dentist a virtual map of your jaw.
What If You Have Low Bone Density?
This is the most common reason people are told “no” by a general dentist. But here is the truth: low bone density rarely means no implant. It usually means preparation.
Three main solutions exist:
1. Bone graft. A dentist adds bone material to your jaw. This can come from your own body (often from your chin or shin), from a donor, or from synthetic materials. Healing takes 4 to 9 months. After that, your bone is thick enough for an implant.
2. Sinus lift. This is a specific type of graft for upper back molars. The maxillary sinus sits just above those teeth roots. When those teeth are missing, the sinus expands into the bone space. A sinus lift pushes the sinus membrane up and adds bone underneath. Success rates exceed 90% for this procedure.
3. Short or narrow implants. Some implants are only 6mm long (standard is 10-12mm). Others are 3mm wide (standard is 4-5mm). These mini implants need less bone. They work well in certain cases, though they may not last as long as standard implants.
Realistic expectation: A bone graft adds 3 to 9 months to your treatment timeline. It also adds 500to3,000 per site. But for many people, this is the difference between “no” and “yes.”
2. Gum Health: The Seal That Protects
You can have perfect bone. But if your gums are infected, the implant will fail.
Gum disease (periodontitis) destroys the attachment between your gums and your teeth. It also eats away at bone over time. An implant placed into infected gums is like planting a tree in a swamp. The roots never hold.
Signs of Unhealthy Gums
- Bleeding when you brush or floss
- Red, swollen, or tender gums
- Persistent bad breath
- Gums pulling away from teeth (recession)
- Loose teeth
The Good News
Gum disease is treatable. Before any dentist places an implant, they will require a periodontal evaluation. If you have active disease, you will need:
- Scaling and root planing – a deep clean below the gumline
- Antibiotic therapy – gels or oral meds to kill bacteria
- Follow-up – a re-evaluation after 4 to 6 weeks
Once your gums are healthy and stable, you can move forward with implants.
Note for current implant holders: Even after placement, gum health matters. Peri-implantitis is an infection around an implant. It is the leading cause of late implant failure. Daily flossing and regular cleanings are not optional. They are everything.
3. Medical Conditions and Medications
This is where many people get nervous. Let us be clear right now: having a medical condition does not automatically disqualify you. It just means your dentist needs to know everything.
Conditions That Require Extra Caution
| Condition | Risk Level | What Helps |
|---|---|---|
| Uncontrolled diabetes | High | Get HbA1c under 7.0% before surgery |
| Osteoporosis | Medium | Review bisphosphonate medications (see below) |
| Autoimmune disease | Medium | Coordinate with your rheumatologist |
| Cancer (active chemo/radiation) | High | Wait until treatment ends |
| Heart disease | Low to Medium | Antibiotics before surgery (per your cardiologist) |
| HIV (controlled) | Low | Normal candidacy with good viral control |
The Bisphosphonate Conversation
This deserves its own section. Bisphosphonates are drugs for osteoporosis (Fosamax, Actonel, Boniva). They also treat some cancers.
These drugs can cause a rare but serious condition called medication-related osteonecrosis of the jaw (MRONJ). The bone does not heal after an extraction or implant.
Here is the honest breakdown:
- Oral bisphosphonates (taken by mouth for less than 4 years) – low risk. Most dentists will proceed with caution.
- Oral bisphosphonates for more than 4 years – moderate risk. A drug holiday (stopping for 3-6 months) may be recommended.
- IV bisphosphonates (for cancer) – high risk. Implants are generally not recommended.
Never stop a medication without your prescribing doctor’s approval. Your dentist and doctor should talk directly.
Diabetes and Implants
Diabetes affects healing and blood flow. But well-controlled diabetics get implants every day.
One study followed 500 diabetics with implants over 10 years. Those with HbA1c under 7.0% had success rates above 95%—nearly identical to non-diabetics. Those with HbA1c above 8.0% had failure rates three times higher.
The message: control your blood sugar first. Then pursue implants.
Smoking and Vaping
Let us be completely honest. Smoking is bad for implants. It reduces blood flow to the gums. It slows healing. It increases infection risk.
Success rates:
- Non-smokers: 95-98% over 10 years
- Smokers (less than 10 per day): 85-90%
- Heavy smokers (10+ per day): 70-80%
Vaping is newer. Early research suggests it also impairs healing, though possibly less than cigarettes. The safest approach is to quit entirely for two weeks before surgery and two months after. Many patients use this as the motivation they needed to stop for good.
4. Age: Young and Old
Children and Teenagers
Here is a firm rule: Do not place dental implants in growing children.
Why? Your jawbone grows until about age 18 in girls and 21-22 in boys. An implant fuses completely with bone—it cannot move. As the rest of the jaw grows, the implant stays where it was placed. This leads to a tooth that looks “sunken” or out of position.
For a child or teen, the better solution is a space maintainer, a partial denture, or a bridge. Once growth stops, implants become an option.
Older Adults
Age alone is never a barrier. Dentists have placed implants in patients over 90 years old. What matters is health, not the number on your birthday cake.
Older adults often have less bone density. But as we covered, bone grafts fix that. They may take multiple medications. But only a few interfere with implant success.
The real consideration for older patients is:
- Can you sit for a 1-2 hour surgery?
- Can you heal for 3-6 months before getting the final crown?
- Can you maintain daily oral hygiene (brushing, flossing)?
If the answer to those is yes, age is not a problem.
Quote from Dr. Lisa Markham, prosthodontist: “My oldest implant patient was 94. She got a lower denture secured by two implants. She told me she could finally eat an apple for the first time in twenty years. Age is just a number.”
5. The Complete Candidacy Checklist
Use this simple checklist to see where you stand. Answer honestly.
| Question | Yes | No | Notes |
|---|---|---|---|
| Do you have one or more missing teeth? | ☐ | ☐ | Implants replace single or multiple |
| Is your mouth free of active gum disease? | ☐ | ☐ | If no, treat first |
| Do you have enough jawbone? | ☐ | ☐ | If no, bone graft may help |
| Do you have a chronic illness? | ☐ | ☐ | If yes, note which one |
| Are you taking any medications? | ☐ | ☐ | Especially bisphosphonates or blood thinners |
| Do you smoke or vape? | ☐ | ☐ | Quitting improves success dramatically |
| Can you commit to 3-9 months of healing? | ☐ | ☐ | This is the typical timeline |
| Do you have 3,000−6,000 per implant? | ☐ | ☐ | Insurance may cover part |
| Will you brush, floss, and see your dentist regularly? | ☐ | ☐ | Maintenance is mandatory |
If you checked “No” for one or two items, you are likely still a candidate—with extra steps. If you checked “No” for four or more, have a detailed conversation with a specialist.
6. Absolute Contraindications (Rare but Real)
Honesty matters. A small percentage of people truly cannot have implants. These are absolute contraindications:
- Untreated, severe osteoporosis with long-term IV bisphosphonates
- Current radiation therapy to the jawbone
- Active, untreated cancer
- Severe uncontrolled bleeding disorder
- Active substance abuse (especially methamphetamine, which destroys oral tissue)
- Active psychiatric condition that prevents informed consent or aftercare
That is the complete list. Notice how short it is. Almost everyone else falls into the “candidate with conditions” category.
7. Partial Candidacy: When You Almost Qualify
This is the most common scenario. You have some strengths and some weaknesses. Let us walk through examples.
Scenario A: Low Bone, Perfect Health
You are 45 years old. You lost a tooth three years ago. You are healthy, non-smoker, great gums. But your X-ray shows significant bone loss.
Verdict: Excellent conditional candidate.
Plan: Bone graft (4 months healing) → Implant placement (6 months integration) → Crown.
Total time: 10 months.
Success probability after graft: 95%+
Scenario B: Moderate Gum Disease, Smoker
You have bleeding gums. You smoke 8 cigarettes per day. You want to replace two missing molars.
Verdict: Conditional candidate with work to do.
Plan: Quit smoking (2 weeks before). Scaling and root planing (6 weeks healing). Re-evaluation. If gums stable, proceed with implants. High risk for complications.
Success probability: 75-80% if you continue smoking. 90%+ if you quit permanently.
Scenario C: Well-Controlled Diabetes, Healthy Otherwise
Your HbA1c is 6.5%. You take metformin. No other issues.
Verdict: Good candidate.
Plan: Standard implant protocol. Coordinate with your endocrinologist. Monitor healing closely.
Success probability: 95%+.
8. Alternatives When Implants Are Not Right (Yet)
Sometimes the answer is “not now.” That does not mean “never.” Here are temporary and permanent alternatives.
| Alternative | Pros | Cons | Best For |
|---|---|---|---|
| Removable partial denture | Low cost (500−1,500) | Uncomfortable, affects taste, can damage adjacent teeth | Temporary solution while you save or heal |
| Fixed bridge | Faster (2-3 weeks) | Shaves down healthy teeth, lasts 10-15 years then replacement | People who want a fixed option but cannot have implants |
| Resin-bonded bridge (Maryland bridge) | Minimal tooth alteration | Less durable for back teeth | Single missing front tooth in low-bite-force area |
| Do nothing | Free | Bone loss continues, adjacent teeth shift | Not recommended |
If you are told you cannot have implants today, ask:
- What specific condition makes me ineligible?
- Can that condition be treated or managed?
- *If I return in 6 months after [treatment], will we re-evaluate?*
A good dentist will welcome these questions.
9. The Financial Reality of Candidacy
Being a candidate also means being able to afford the process. Let us be real about numbers.
Typical Costs in the United States (2025 estimates)
| Procedure | Cost Range |
|---|---|
| Single implant + abutment + crown | 3,000−6,000 |
| Bone graft (per site) | 500−3,000 |
| Sinus lift | 1,500−3,000 |
| CBCT scan | 200−500 |
| Implant-supported denture (full arch) | 15,000−30,000 per arch |
| All-on-4 (full mouth restoration) | 25,000−50,000 per arch |
Insurance coverage is limited. Most dental plans cover 1,000to1,500 per year total. They may cover the crown but not the implant itself. Some medical insurance covers bone grafts if they are “medically necessary” (rare).
Financing Options
- CareCredit – medical credit card. Promotional financing available.
- LendingClub – personal loans for dental work.
- Dental schools – 30-50% lower costs. Treatment is slower but supervised by experts.
- Dental tourism – Mexico, Costa Rica, Colombia offer implants for 800−2,000. This carries risks with follow-up care.
Important note: Cheap implants are not good. Good implants are not cheap. If a deal seems too good to be true, ask about the implant brand, the surgeon’s training, and the warranty.
10. The Timeline: From First Visit to Final Bite
Knowing what to expect reduces anxiety. Here is a realistic timeline for a straightforward case with no complications.
Month 1 – Evaluation
- Consultation, X-rays, CBCT scan
- Medical history review
- Treatment plan discussion
Month 2 – Preparation (if needed)
- Bone graft or sinus lift (adds 3-9 months)
- Gum disease treatment (adds 1-2 months)
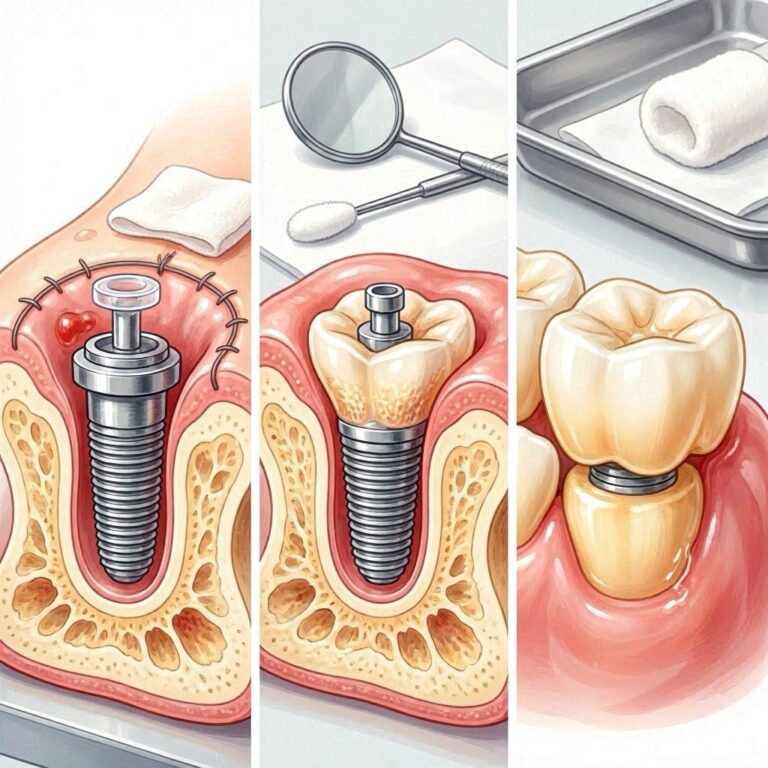
Month 3 – Implant Surgery
- Local anesthesia (or sedation if desired)
- Implant placed into bone
- Healing cap or temporary tooth (if needed)
Months 3 to 9 – Osseointegration
- The bone grows around the implant
- You wear a temporary partial or nothing
- Soft foods recommended for first 2 weeks
Month 9 – Abutment Placement
- Minor surgery to expose implant
- Attach abutment (the connector piece)
- Impressions for final crown
Month 10 – Final Crown
- Crown screwed or cemented onto abutment
- Bite adjustment
- You leave with a new tooth
Total: 10 to 14 months for a grafted case. 4 to 7 months for a non-grafted case.
11. Success Rates by Category
Real numbers help you make real decisions.
| Patient Category | 5-Year Success Rate | 10-Year Success Rate |
|---|---|---|
| Healthy non-smoker, good bone | 98% | 96% |
| Well-controlled diabetic | 95% | 93% |
| Smoker (<10/day) | 88% | 82% |
| Heavy smoker (10+/day) | 78% | 70% |
| After bone graft | 95% | 93% |
| After sinus lift | 94% | 91% |
| Osteoporosis (no bisphosphonates) | 94% | 92% |
| Full-mouth All-on-4 | 97% | 95% |
These numbers come from long-term studies (over 10,000 implants tracked for a decade).
12. Questions to Ask Your Dentist About Your Candidacy
You are the consumer. Ask these questions at your consultation.
- “Based on my CBCT scan, how much bone do I have in height, width, and density?”
- “Do you perform bone grafts in-office, or would you refer me to a specialist?”
- “What brand of implant do you use? How long is the warranty?”
- “What is your personal success rate with patients like me?”
- “What are the signs of failure I should watch for at home?”
- “If the implant fails in the first year, what is your policy on replacement?”
- “Can you show me before-and-after photos of cases similar to mine?”
A confident, ethical dentist answers these without hesitation.
13. Red Flags: When to Get a Second Opinion
Not every dentist gives good advice. Look for these warning signs.
- “You need implants right now or your teeth will collapse.” – This is fearmongering. Missing teeth do cause changes, but you usually have months to decide.
- “We never do bone grafts. They don’t work.” – False. Grafts have decades of research.
- “Everyone is a candidate. I’ve never seen a failure.” – Also false. Every implant dentist has seen failures.
- Price that is half the average with no explanation. – Proceed with extreme caution.
- Pressure to sign same day. – Legitimate implant planning takes time. No ethical dentist rushes you.
If you hear any of these, walk out. Get a second opinion from a prosthodontist or oral surgeon.
14. Maintaining Your Candidacy After Implants
You earned your implant. Now keep it.
Daily home care:
- Brush twice a day (soft bristles)
- Floss around the implant specially (use superfloss or implant floss)
- Consider a water flosser on low pressure
- Avoid chewing ice or hard candy
Professional care:
- Cleanings every 6 months
- Annual X-ray to check bone levels around implant
- Bite check once per year
Lifestyle:
- If you smoke, quit. It is the #1 cause of late failure.
- If you grind your teeth, wear a nightguard.
- See your dentist at the first sign of bleeding or pain around the implant.
An implant is not a set-it-and-forget-it solution. It is a partnership between you and your dentist. The patients who follow these rules keep their implants for 30+ years.
Conclusion
Dental implant candidacy is rarely a simple yes or no. It is a conversation about your bone, your gums, your health, and your goals. Most people who want implants can get them—sometimes with a little preparation like a bone graft or gum treatment. Age is almost never a barrier, and even conditions like diabetes or osteoporosis usually allow implants when well-managed.
The keys to success are honest evaluation, realistic expectations, and a commitment to daily care. If you take those three things seriously, there is an excellent chance you will be enjoying a stable, natural-looking implant for decades to come.
FAQ: Dental Implant Candidacy
Q1: Can I get an implant if I have receding gums?
Yes, but the recession may need treatment first. If gum disease caused the recession, treat that. If recession is mild, implants are still possible.
Q2: How long after tooth extraction can I get an implant?
You have three options: immediate placement (same day), early placement (4-8 weeks), or delayed placement (4-9 months). Each has pros and cons. Your dentist will recommend based on your bone and infection risk.
Q3: Do dental implants hurt?
The surgery is done with local anesthesia. You feel pressure, not pain. Afterward, most people describe soreness similar to a tooth extraction for 3-5 days. Over-the-counter pain relief usually suffices.
Q4: Can I have an MRI if I have a dental implant?
Yes. Dental implants are made of titanium or zirconia, both non-magnetic. They are safe for MRIs. However, they may create a small artifact (blurring) on images near the implant.
Q5: Are dental implants covered by Medicare or Medicaid?
Original Medicare does not cover dental implants. Some Medicare Advantage plans offer limited dental benefits. Medicaid coverage varies by state; most states do not cover implants except for rare medical necessity.
Q6: What happens if an implant fails?
Your dentist will remove it (simple procedure), allow the bone to heal for 2-4 months, and then you can try again. Success rates for second attempts are still high—around 90% with careful planning.
Q7: Can I get an implant years after losing a tooth?
Yes. You will likely need a bone graft because the bone has resorbed. But time alone is not a disqualifier.
Q8: Do I need a referral to see an implant dentist?
No. You can directly schedule with a periodontist, oral surgeon, or prosthodontist. General dentists also place implants but may refer complex cases.
Q9: Can I get implants on both top and bottom?
Yes. Many people get full-mouth restoration. The surgery may be staged (one arch at a time) or done together. Healing takes longer, but the result is life-changing.
Q10: How do I find a good implant dentist?
Look for a specialist (prosthodontist, periodontist, oral surgeon) who places at least 50 implants per year. Read reviews. Ask about their warranty. Check if they use CBCT scanning. Trust your gut.
Additional Resource Link
For a directory of board-certified prosthodontists in your area, visit the American College of Prosthodontists:
👉 www.gotoapro.org
This resource helps you find a specialist who has completed three additional years of training beyond dental school focused on implants and tooth replacement.