Do Veneers Have Dental Health Benefits
Walk into any modern dental practice, and you will likely see brochures showcasing stunning smile transformations. The images are striking. Worn, chipped, or discolored teeth become perfectly uniform and brilliantly white. For many people, this represents the ultimate aesthetic goal. But behind the glossy photos, a far more important question often goes unasked. Do veneers have dental health benefits, or are they simply a cosmetic luxury?
The short answer surprises many. Yes, dental veneers can offer real, functional health advantages. However, this truth comes with a very important nuance. These benefits depend entirely on the material chosen, the skill of the dentist, and the patient’s commitment to care. A poorly executed veneer offers zero protection. In fact, it can create a nightmare of decay and gum disease. A well-made, properly bonded veneer, on the other hand, acts like a shield and a support system for a compromised tooth.
This guide strips away the marketing hype. We will explore the biomechanical protection a thin porcelain shell provides. We will look at how veneers replace lost enamel function. We will examine the connection between a straight smile and gum health. You will learn when a veneer protects a tooth and when it simply disguises a problem that still needs real treatment.
Crucially, we avoid false promises here. A veneer will not stop you from getting cavities on other teeth. It will not cure gum disease. But if you have specific structural damage, erosion, or minor misalignment, the health benefits can be life-changing. Let’s move beyond the idea of a “Hollywood smile” and explore the genuine therapeutic value of this misunderstood dental treatment.
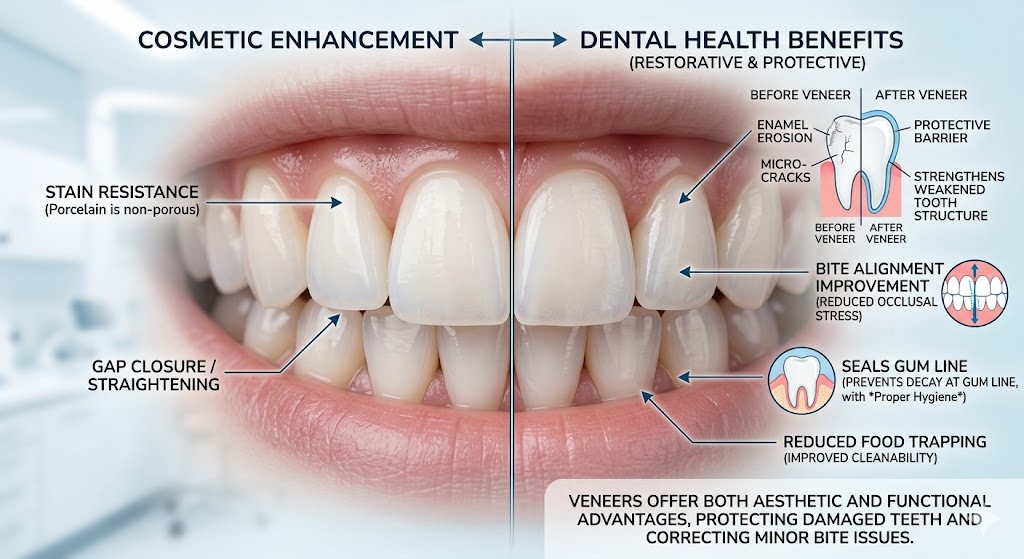
The Dual Nature of Veneers: Cosmetic Meets Functional
Dentistry rarely draws a clean line between beauty and health. A filling on a front tooth must match the color of the enamel. A crown must look natural while bearing the full force of your bite. Veneers sit right at this intersection, perhaps more than any other procedure.
Understanding the Prosthetic as a Protective Layer
Think of a natural, healthy tooth. The outer shell, the enamel, acts as a helmet. It is the hardest substance in the human body. It resists the impact of chewing, shields the sensitive dentin underneath, and insulates the nerve from temperature extremes. However, enamel does not grow back. Once acid erosion, grinding, or an accident wears it away, the softer dentin lies exposed. Dentin is filled with microscopic tubules that lead directly to the nerve. When dentin is bare, cold water hurts. A spoon of hot soup sends a jolt. And bacteria have a far easier path to the pulp.
A dental veneer, when we use it functionally, acts as a synthetic enamel replacement. We bond a thin layer of ceramic or composite to the front of the tooth. This layer takes over the shielding role of the missing natural enamel. It seals the tubules. It insulates against heat and cold. It provides a hard, smooth surface that resists new acid attacks better than weakened, pitted natural enamel.
“Patients often arrive thinking only about the color,” explains a restorative dentist with over two decades of experience. “They leave realizing the veneer stopped the cold sensitivity they had lived with for years. The aesthetic change is what they see in the mirror. The health change is what they feel at the dinner table.”
This duality changes the discussion entirely. You do not seek veneers just to get a better Instagram photo. You seek them to replace lost function.
When a Veneer Corrects More Than Just Shape
A tooth with a small chip on the corner is more than an aesthetic annoyance. That sharp, irregular edge can scrape the inside of your lip or the side of your tongue. Over time, the chronic irritation can lead to a traumatic fibroma or a persistent ulcer. A veneer smooths the edge and covers the defect. It transforms the tooth from a source of soft-tissue damage into a neutral, harmless structure.
Similarly, consider a tooth with a deep pit or a structural groove in the enamel. These areas collect biofilm far more aggressively than a smooth surface. Some people inherit these developmental imperfections. No matter how well they brush, the groove remains a plaque trap. A veneer resurfacing the front of the tooth eliminates the microscopic crevice. The smooth ceramic becomes a hostile environment for bacterial attachment. This does not mean you can ignore hygiene. It simply levels the playing field for those with challenging enamel anatomy.
Enamel Replacement: The Core Functional Benefit
If we strip the conversation down to pure physiology, the primary health benefit of a veneer is the restoration of a protective hard-tissue layer. Let’s look at the specific conditions where this really matters.
Dental Erosion and the Veneer Shield
Dietary acids present one of the greatest threats to modern dentition. Citrus fruits, sparkling water, sports drinks, and even some herbal teas expose teeth to a low-pH environment. The enamel surface demineralizes. Saliva tries valiantly to neutralize the acid and remineralize the crystals, but chronic exposure overwhelms the system. The enamel becomes thin, translucent at the edges, and eventually cupped out, revealing the yellowish dentin beneath.
When the erosion is still moderate and primarily affects the front surfaces, porcelain veneers offer a brilliant intervention. The dentist removes a fraction of a millimeter of the already compromised enamel and bonds the ceramic restoration. This ceramic is essentially inert. It does not demineralize in acid. It does not erode. For a patient with a history of severe acid wear, this is a protective upgrade. The underlying tooth structure, protected by the bonded veneer, no longer faces direct acid attack.
A word of caution, however. The back of the tooth remains uncovered. If the patient continues to sip acidic drinks all day, the palatal surface will continue to erode. A veneer is a shield on one side, not a full-coverage helmet like a crown. The patient must address the root cause of the erosion to achieve lasting health. The veneer simply provides a durable front-line defense.
Protecting Dentin and Reducing Sensitivity
Dentin hypersensitivity affects a significant portion of the adult population. The sharp, sudden pain upon exposure to cold, sweet, or even a breath of cold air can make eating and drinking miserable. Desensitizing toothpastes work for many by blocking the tubules with minerals like potassium nitrate or stannous fluoride. But for some, the enamel loss is too great.
Here, the veneer becomes a medical device. The adhesive process for modern veneers creates a hybrid layer between the tooth and the ceramic. The resin cement infiltrates the exposed dentin surface, physically plugging the tubules. Then the ceramic itself provides a thick, insulating barrier. The result often proves immediate and dramatic. A patient who could not bite into ice cream suddenly enjoys it pain-free.
“After my veneers, I cried because I could drink a cold glass of water without wincing,” one patient shared in a long-term outcome study. “I went in for the look and came out with my life back.”
This aspect of treatment is undeniably a dental health benefit. Chronic pain has a massive impact on quality of life, nutrition, and even sleep if sensitivity keeps someone from eating or drinking properly before bed. When veneers resolve that pain, we classify them as functional therapy, not elective cosmetics.
A Closer Look at Minor Misalignment and Oral Hygiene
Crowded teeth cause more than an uneven smile. They create overlapping surfaces that your toothbrush and floss cannot easily reach. The plaque that accumulates in these hidden zones calcifies into tartar. The tartar harbors bacteria that trigger gingivitis, and over time, periodontitis. Bone loss follows, and teeth loosen. The cosmetic problem of crookedness evolves into a serious medical condition.
Closing Gaps and Preventing Food Impaction
A diastema, a gap between the front teeth, has cultural and aesthetic appeal for some. For others, it creates a consistent annoyance. Food, particularly fibrous items like lettuce or meat, wedges between the teeth at every meal. Constant food impaction does two things. It forces the patient to use toothpicks or fingernails, which can traumatize the papillae, the little triangles of gum between the teeth. And the retained food ferments, feeding a localized bacterial bloom. The gum in that spot becomes chronically red and bleeds easily.
Veneers can close a small-to-moderate diastema. By carefully widening the mesial and distal contours of the adjacent teeth, the dentist creates contact where none existed. The teeth now naturally deflect food away from the gum. There is no more packing. The gum tissue gets a chance to heal. The patient can floss normally without shredding floss in a tight, abnormal contact. This represents a genuine periodontal health improvement.
Smoothing Over Rotated or Ridged Teeth
A tooth rotated even fifteen degrees out of alignment creates a plaque-retentive corner. The patient aims their brush straight on, but the twisted anatomy leaves a shadowed zone on one side. Over months, a line of inflammation tracks right down the side of the root. This localized gum inflammation, if left unchecked, can progress to a bony defect.
Porcelain veneers can sometimes optically and structurally correct these mild rotations. Instead of moving the root through bone with months of orthodontics, the dentist reshapes the visible portion of the tooth. The new, properly contoured surface aligns with the arch. The shadow zone disappears. The patient can now brush effectively. The gum responds within a week, shrinking back to a firm, pink, knife-edged state.
Let’s be honest and precise here. This does not correct the root position. Severe crowding that compromises the attachment of the gum or the bite still requires orthodontics. But for a mild problem that purely affects cleansability, a carefully designed veneer can serve as a valid therapeutic tool.
Important Note: Veneers should never be your first option for treating periodontal disease. If you have active gum infection, bleeding on probing, and deep pockets, get that under control first. A veneer placed in an inflamed environment will trap more plaque and make the situation worse. Periodontal health must be achieved before any adhesive restoration.
Dental Material Science: Choosing Health Over Hype
Not all veneers are created equal when we talk about long-term oral health. The choice of material directly dictates how the restoration interacts with the gum tissue, how it wears, and how plaque adheres.
Porcelain Versus Composite Resin: A Health-Focused Comparison
The dentist presents you with two main options: ceramic (almost always a glass-ceramic like lithium disilicate) or composite resin applied directly to the tooth. You might focus on the cost difference. The health implications matter more.
| Feature | Porcelain (Ceramic) Veneers | Composite Resin (Direct) Veneers |
|---|---|---|
| Surface Finish After Polishing | Extremely smooth, glazed surface. Bacteria struggle to adhere. | Can be polished well, but surface degrades slightly over time, becoming rougher. |
| Plaque Accumulation Tendency | Very low. Resists biofilm formation similar to intact enamel. | Moderate. More prone to biofilm formation at the microscopic level. |
| Gum Tissue Response | Often excellent. Well-finished margins allow the gum to form a tight seal. | Can be good, but porosities and rougher margins can trap stain and plaque, causing localized inflammation. |
| Stain Resistance | Impervious to coffee, tea, and red wine stains. | Absorbs pigments over time. The color change is unhygienic looking, but more importantly, the surface becomes stickier for plaque. |
| Durability Under Force | Very high. A properly bonded ceramic veneer becomes part of the tooth structure. Chipping is rare but possible with trauma or parafunction. | Moderate. Chips and wears down more readily. Worn composite creates a step at the margin that catches plaque. |
| Repairability | Difficult. A broken porcelain veneer usually means replacement. | Easy. The dentist can add more composite and polish it chairside. |
For someone serious about maximizing oral health, the data leans decisively toward well-made porcelain. The glazed surface mimics healthy enamel’s low-plaque affinity. The gum likes it. The margin, if placed correctly by the dentist, seals so tightly that bacteria cannot penetrate. Composite has its place, particularly in young patients where we want to be extremely conservative and when budget constraints are severe. But we must acknowledge that composite requires more meticulous hygiene and professional maintenance to keep the gum healthy over a decade.
The Supragingival Margin Principle
One of the single most important health decisions a dentist makes during veneer preparation involves the margin. This is the line where the veneer meets the tooth. A margin placed below the gumline, in what we call the subgingival zone, risks violating the biological width. The biological width is the body’s defense space. When a restoration margin invades it, the gum rebels with chronic inflammation. Bleeding, recession, and even bone loss can occur.
A health-focused, conservative dentist places the veneer margin just at or above the gumline whenever possible. This is the supragingival margin. It allows the patient to see the edge and clean it perfectly. It does not impinge on the delicate gum attachment. The tissue stays calm and pink. Some dentists argue a subgingival margin is needed for aesthetics on a smile where a lot of gum shows. But with modern ceramics that mimic the optical properties of enamel, a skilled ceramist can hide an equigingival margin so well that only a microscope would reveal it. Insist on a conservative margin placement. Your periodontal health depends on it.
Bite Stabilization and the Protective Role of Veneers
Your back teeth do the heavy grinding and chewing. Your front teeth guide the jaw. When you move your jaw side to side, your canines and incisors should ideally slide against each other in a way that gently separates the back teeth. This is called canine guidance or anterior guidance. It protects the back teeth from excessive lateral forces and clenching damage. When the front teeth are worn, broken, or misaligned, this protective system fails.
Restoring Anterior Guidance Through Restorative Design
A patient presents with severe wear on their upper front teeth from years of grinding. The teeth are short, flat, and chipped. The dentist rebuilds the length and the palatal contours with porcelain veneers. But they do not just build them to look nice. They design the inclines so that when the patient moves their jaw forward and to the side, the lower teeth smoothly contact the new porcelain surfaces and instantly lift the back teeth apart. The heavy muscles of mastication get a signal to relax. The posterior teeth, already worn, receive a reprieve from night-time parafunction.
This is highly specialized work. It requires an understanding of occlusion, the way the teeth meet. A purely cosmetic dentist who ignores function might create veneers that look beautiful but trap the jaw in a traumatic bite. The patient would then develop jaw pain, headaches, and chipped porcelain. A functional, health-focused restorative dentist uses the veneer process as an opportunity to rebuild the protective architecture of the mouth.
“We’re not just putting white shells on teeth,” a prosthodontist with a focus on full-mouth rehabilitation says. “We’re reprogramming the muscles and protecting the entire stomatognathic system. The anterior restorations become the canary in the coal mine. If we do them right, everything stays healthier.”
Protecting Weakened Teeth From Fracture
A tooth with a large, old composite filling on the front corner lives under constant stress. Every bite forces the remaining tooth structure to flex. Enamel is brittle. It doesn’t bend. Over time, microfractures radiate from the edge of the filling. One day, a bite on an olive pit or a crusty piece of bread causes a catastrophic corner fracture. Now the tooth needs a much larger restoration or even a crown.
A porcelain veneer bonded over the entire front surface of such a tooth acts like a splint. The adhesive creates a monoblock: a single unit combining tooth and ceramic. The chewing forces distribute more evenly across the whole facial surface. The concentration of stress at the corner dramatically reduces. Studies using finite element analysis confirm this. A bonded ceramic restoration strengthens a compromised anterior tooth. It does not weaken it.
This preservation of natural tooth structure represents the pinnacle of healthy dentistry. We avoid the cycle of ever-larger fillings, root canals, and extractions. We keep the nerve alive. We keep the biological tooth root in the bone. No implant, no bridge, can match the proprioceptive feedback of a natural, healthy tooth root.
The Psychological and Systemic Connection
We cannot separate oral health from mental and systemic health. The mouth is not a disconnected white box sitting outside the body. Inflammation here travels everywhere. And how you feel about your teeth dictates how you eat, speak, and socialize. These are health outcomes, every bit as real as a bleeding pocket measurement.
Nutrition and the Willingness to Eat Whole Foods
Consider the patient with sensitive, broken, or unsightly teeth. They self-select soft, processed foods. They choose white bread over a crusty whole-grain roll. They skip the apple and the carrot sticks. They avoid the salad with crunchy nuts. Their diet becomes one of mush. Fiber intake drops. Nutrient diversity plummets. This directly impacts gut health, cardiovascular health, and glycemic control.
When veneers restore confidence and eliminate sensitivity, these patients re-engage with a whole-food diet. The ability to bite into a crisp apple without fear is a health intervention. The pleasure of chewing a fresh salad contributes to a healthier microbiome. While no dentist prescribes veneers simply to improve diet, the behavioral outcome is a legitimate benefit. Function restores nutrition.
The Elimination of Chronic Low-Grade Pain
Earlier, we discussed severe sensitivity. But even mild, chronic discomfort changes behavior. You chew on one side. You hold your jaw differently. You create a muscle imbalance that leads to tension headaches radiating from the temples. Removing the source of oral discomfort can resolve these secondary myofascial pains. The veneer thus acts indirectly as a pain management tool. Not because it has any pharmacological action, but because it removes the noxious stimulus that caused the guarding and asymmetrical function.
The Biological Price of Veneers: A Balanced Assessment
An honest guide requires balance. We have outlined the compelling health benefits veneers can offer. But this procedure involves an irreversible biological cost. Anyone claiming veneers are purely “healthy” without acknowledging this loses all credibility.
The Irreversible Nature of Tooth Preparation
Even the most conservative “no-prep” or minimal-prep veneer requires some roughening of the enamel surface for the bond to work. In many cases, the dentist removes between 0.3 and 0.5 millimeters of facial enamel. This enamel is gone forever. The body cannot regenerate it. The tooth will never exist without a restoration again. If a veneer debonds, decays, or the patient simply decides they dislike the look in twenty years, they must replace the veneer. The tooth is now in a restorative cycle for life.
This reality demands that we treat the decision with gravity. A healthy tooth with thick, vibrant enamel does not benefit from having that enamel sliced away to make room for a ceramic shell. The structural sacrifice outweighs any marginal gain in plaque resistance. For a tooth already compromised by erosion, wear, or multiple fillings, the sacrifice of a small amount of already-damaged enamel yields a large return in protection. The calculation changes completely.
Potential Risks and How to Mitigate Them
When a veneer fails, it creates serious health problems. Here are the risks and the clinically proven strategies to avoid them.
- Recurrent Decay: The margin can collect plaque. Bacteria produce acid. The enamel at the edge dissolves.
- Prevention: Meticulous oral hygiene, daily use of a fluoridated mouthwash, and keeping margins supragingival.
- Gum Inflammation and Recession: Overcontoured veneers that stick out too far create a shelf that traps food. The body responds with inflammation, and the gum creeps down the root.
- Prevention: Choose a dentist who values emergence profile and biological width. A perfectly contoured veneer looks like a natural tooth emerging from the gum.
- Debonding: The veneer pops off, usually because of inadequate isolation during bonding or parafunction like grinding.
- Prevention: Moisture control with a rubber dam, a strict bonding protocol, and wearing a nightguard if you grind.
- Porcelain Fracture: A heavy bite or an unlucky impact chips the ceramic.
- Prevention: Careful occlusal design, a nightguard, and avoiding using your teeth as tools.
A Critical Note on the Nightguard
I want to highlight the nightguard specifically. If you invest in porcelain veneers and your dentist identifies signs of clenching or grinding, wear the nightguard. Every night. The health of your restorations, the health of the opposing natural teeth, and the health of your jaw joint depend on it. The nightguard acts as a sacrificial bumper, absorbing the paranormal forces that would otherwise chip the porcelain and overload the bond. Do not let a thousand-dollar smile fail for want of a few hundred dollars of acrylic.
The Candidacy Checklist: Will Veneers Improve Your Oral Health?
Veneers are not a universal health tonic. For some, they offer immense protection. For others, they represent an unjustifiable risk. Work through this checklist honestly.
Strong Candidates for Functional Benefit
You fit into this category if:
- You have moderate to severe enamel erosion on the front faces of your teeth from acids.
- Your teeth have numerous enamel defects, chips, or cracks that catch floss and trap plaque.
- You suffer from dentin hypersensitivity that has not responded to desensitizing agents.
- You have a small diastema or mild crowding causing chronic food impaction and gum bleeding that hygiene cannot solve.
- A previous large composite filling is failing, and the remaining tooth structure is thin and at risk of corner fracture.
Poor Candidates or High-Risk Situations
You should seriously reconsider or postpone veneers if:
- You have active, untreated periodontitis with bleeding gums and deep pockets. Treat the disease first.
- You have a high caries rate, meaning you get new cavities every year. Veneers will simply get decayed around the edges.
- You have a severe parafunctional habit like heavy grinding that you refuse to manage with a nightguard.
- Your teeth are perfectly healthy, thick, and strong, and your only concern is a minor aesthetic preference. The removal of healthy enamel is difficult to justify.
- You have an unstable bite that causes jaw pain and clicking. Veneers without occlusal therapy could lock in a dysfunctional bite.
Important Note: A truly ethical dentist will refuse to put veneers on a mouth riddled with active decay. Run from any professional who agrees to do so without a comprehensive plan to stabilize disease first. They are prioritizing their wallet over your long-term well-being.
Long-Term Maintenance as a Health Strategy
Viewing the day your veneers are bonded as the finish line is a mistake. It is the starting line for a new chapter of meticulous care. The health benefits you gained will erode quickly without a maintenance protocol.
The Daily Routine for Longevity and Gum Health
Buy a soft or extra-soft toothbrush. Hard bristles and abrasive toothpaste can scratch the glazed surface of porcelain and cause gum recession at the margin. Brush at the gumline with a forty-five-degree angle, covering just two teeth at a time. Be systematic. Rushing leaves plaque at the critical margin zone.
Floss at least once a day, but ideally after each meal. The floss should slide between the teeth and wrap around the side of the veneer. Do not snap it. Polish the sides of the restoration and rub gently just below the gumline. This removes the biofilm that causes margin decay and papilla inflammation.
Consider adding a water flosser to your toolkit. For patients with multiple veneers, a water flosser with a non-abrasive tip can flush out debris from the gum sulcus in a way string floss cannot reach. It massages the tissue, promoting a tight, healthy cuff around each restoration.
The Role of Professional Maintenance
You need to see your hygienist and dentist on a strict recall schedule. For a patient with an intact, healthy natural dentition, a twelve-month recall might suffice. For a patient with multiple adhesive restorations, a six-month recall is far wiser. The hygienist uses non-abrasive polishing paste and specialized scalers to clean the margins without scratching the ceramic. The dentist checks every margin with an explorer for any sign of a catch, a gap, or early decay. They examine the bite on articulating paper to detect any new high spots from shifting teeth.
Catching a small marginal stain early often allows a simple polish and seal. Ignoring it means decay creeps under the veneer, and the entire restoration requires replacement. Maintenance visits are your long-term insurance policy. Do not skip them.
Cost Versus Health Value: A Long-Term Analysis
Talking about money in a health article feels crass, but financial reality impacts health decisions. Veneers are a significant investment. Understanding the health return on that investment guides a wise choice.
Comparing the Lifecycle of Different Options
Let’s look at a tooth with a compromised facial surface. It could be restored with a direct composite, a porcelain veneer, or left with no treatment beyond monitoring. Over a thirty-year period, the costs and biological impacts diverge significantly.
| Treatment Path | Initial Biological Cost | Average Longevity | 30-Year Maintenance and Likely Interventions | Cumulative Biological Impact |
|---|---|---|---|---|
| No Treatment (Monitor) | None. | Tooth may remain stable or suffer further erosion, wear, or catastrophic fracture. | Possible need for root canal and crown if fracture occurs. | Low initially, but risk of sudden high biological cost if tooth fractures. |
| Direct Composite Veneer | Very low. Minimal enamel roughening. | 5-7 years. | Replacement every 5-7 years. Each replacement removes a tiny bit more enamel and brings new risk of margin decay. | Accumulative over time. By the third replacement, the enamel is significantly thinner, and the tooth may need a crown. |
| Porcelain Veneer | Low to moderate. 0.3-0.5mm enamel removed. | 15-20 years, often longer. | Possible recementation if minor debond. Eventual replacement after two or more decades. The second veneer typically still leaves enough enamel for a strong bond. | Front-loaded biological cost, but very low annualized biological maintenance. Provides definitive, long-lasting protection. |
For the right candidate, the porcelain veneer offers the lowest lifetime biological burden. The initial enamel sacrifice seems like a steep price, but it buys two decades or more of protection. The composite path, while gentler initially, subjects the tooth to repeated interventions, each one inching closer to the nerve. This cumulative trauma often leads to a pulpal problem down the road.
The Intangible Health Investment
Then there is the health value beyond the single tooth. A patient whose anterior guidance is restored, whose diet improves, and whose chronic pain resolves experiences a systemic health dividend that no spreadsheet can quantify. The elimination of a pain trigger improves sleep, lowers cortisol, and enhances immune function. These links are real and documented in the literature on chronic pain and stress physiology. The mouth is a powerful input to the central nervous system. Fix the input, and the output improves.
The Critical Importance of the Dental Team
All these health benefits depend on one variable: the hands and brain of the clinician. Veneer therapy performed poorly is actively dangerous. Veneer therapy performed masterfully is one of the most elegant and health-preserving procedures in restorative dentistry.
The Ceramist as a Health Partner
You may never meet the dental technician who fabricates your veneers, but their skill directly impacts your gum health. A ceramist who layers porcelain with perfect marginal adaptation creates a seamless transition. The margin is almost undetectable. A ceramist who overbuilds the margin creates a small ledge. The ledge catches plaque. The gum bleeds. The ceramist who understands natural tooth anatomy builds subtle lobes and developmental grooves that deflect food correctly. The ceramist who simply makes a shiny white chiclet creates a plaque-retentive, unnatural surface.
Ask your dentist who makes their veneers. A prosthodontist typically works with a master ceramist whose lab fee reflects decades of expertise. This is not an area to seek a bargain. The health of your gums, for the next two decades, rests in the hands of that technician as much as in your dentist’s hands.
Why a Cone Beam CT Matters for Complex Cases
Advanced imaging is not overkill for a full-mouth veneer case. A cone beam computed tomography (CBCT) scan shows the dentist your root positions, the thickness of the bone around each tooth, and the exact location of the nerves. If a tooth needs orthodontic movement before veneers, the CBCT ensures the root does not move out of the bone envelope. If a tooth has a subclinical root fracture, it shows up before the dentist cuts the tooth down. The scan also reveals airway patency. A constricted airway contributes to mouth breathing, which dries the enamel and promotes decay around margins. Comprehensive health-focused treatment evaluates all of this.
Debunking Common Myths About Veneers and Health
Misinformation scares people away from beneficial treatment or pushes them toward unnecessary procedures. Let’s clear up the most persistent falsehoods.
Myth 1: “Veneers Ruin Your Teeth”
The reality: Poorly planned, poorly executed veneers ruin teeth. That is true. A careless dentist who buries margins deep under the gum, creates bulky overcontours, or bonds over decay sets the teeth on a path to destruction. Well-executed veneers on appropriate teeth strengthen and protect them. The bonding process, using modern adhesive techniques, actually increases the fracture resistance of a compromised tooth. The statement “veneers ruin your teeth” is like saying “cars kill people.” A well-built car driven responsibly is safe. A wreck with a drunk driver is deadly. The tool is not the problem. The operator is.
Myth 2: “You Can’t Get Cavities With Veneers”
This is dangerously wrong. The porcelain itself cannot decay. No bacteria can burrow into the ceramic. But the tooth structure behind the porcelain, and especially the margin where the porcelain meets the tooth at the gumline, is completely vulnerable. If you neglect hygiene, plaque sits on that junction. The acid decalcifies the natural enamel at the edge. The decay can tunnel underneath the veneer, silently destroying the tooth while the smile still looks perfect on the surface. By the time the patient notices a dark line or feels a catch, the decay might have reached the nerve. Veneers demand the same rigorous hygiene as natural teeth, perhaps even more care at the gumline margin.
Myth 3: “Porcelain Is Always the Healthiest Choice”
We talked about the plaque affinity. Porcelain is superior to composite in that regard. But consider a young patient with a single, very small chip on a tooth with otherwise magnificent, thick enamel. Preparing that tooth for a porcelain veneer to fix a 1-millimeter corner would be biologically criminal. A minuscule composite bonding, requiring zero tooth reduction, preserves the natural enamel and still smooths the chip. The healthiest material is the one that respects the biological cost. Sometimes, the most conservative choice is the healthiest, even if the material itself is technically inferior in laboratory tests.
Myth 4: “Veneers Protect Against Gum Disease”
Veneers do not have any antimicrobial properties that protect against periodontitis. If you had gum disease before, you are still susceptible. What they can do is make hygiene easier if they correct crowded, twisted, or deeply grooved anatomy that previously trapped bacteria. The smooth, properly contoured porcelain allows the gum to form a tight seal and the patient to brush effectively. This reduces plaque accumulation, which reduces the risk of gum inflammation. So, indirect protection through improved cleansability—yes. Direct protection or immunity—absolutely not.
A Lifelong Perspective: Age, Wear, and Adaptation
Your mouth is not static. Teeth shift. Gums recede slightly with age. Bite forces change as back teeth wear or are lost. A veneer case must be designed with this future reality in mind.
Planning for the Aging Smile
A health-conscious dentist designs veneers that will still look and function well when you are seventy. They avoid an aggressively white, opaque shade that will look grotesque against an aging face with naturally darker natural teeth. They build the bite so that as the natural teeth wear slightly, the porcelain does not become a dominant interference point. They prepare the margins in a way that, if the gum recedes a millimeter over forty years, the tooth at the new gumline still has healthy enamel and no exposed margin. This long-range thinking separates the true clinician from the smile-mill technician.
Managing Replacement and Failure
You must accept that one day, your veneers will need replacement. A healthy perspective sees this not as a failure, but as the natural lifecycle of a prosthetic. The goal is to make that lifecycle as long as possible and the replacement minimally traumatic. When a dentist removes an old veneer on a tooth that was prepared conservatively, they find healthy, hard, wet dentin. The tooth has been protected. The replacement is straightforward. When a dentist removes a veneer that was heavily cut with deep margins and exposed dentin, the tooth is weak, possibly decalcified, and the prognosis declines. Choose a clinician who makes the initial preparation a work of long-term preservation, not just expediency.
Navigating the Decision: A Patient’s Guide
If you are considering veneers and the health dimension is important to you, take these concrete steps.
- Comprehensive Exam First. Insist on a full-mouth series of radiographs, a periodontal charting with pocket depths, an occlusal analysis, and a caries risk assessment. The health of the foundation must be established before the renovation begins.
- Ask the Hard Questions. Look your dentist in the eye and ask:
- “Will you place my margins above the gumline?”
- “How will you manage my bite to protect the porcelain and my joints?”
- “Do you have a protocol to prevent decay at the margins long-term?”
- “May I see cases of yours that are ten years old?”
- Seek a Functional Expert. Consider a prosthodontist. These are dentists who specialize in complex restoration and occlusion after an additional three years of training. For a case involving multiple teeth, their expertise often delivers a healthier, longer-lasting result.
- Visualize the Mock-up. A diagnostic wax-up and a temporary mock-up in the mouth are not just for approving aesthetics. You wear the new shape. You feel if the bite is comfortable. You assess if you can clean around the new contours. If the mock-up creates speech issues or gum pressure, the final veneers will too. The mock-up is your functional test drive. Do not skip it.
Summary and Conclusion
Dental veneers transcend the simple label of cosmetic dentistry when applied with biological intelligence. For teeth compromised by acid erosion, structural cracks, or chronic sensitivity, a porcelain veneer acts as a permanent, durable layer of artificial enamel. It restores protective guidance to the jaw, shields exposed dentin, and creates smooth, cleansable surfaces that support the health of the surrounding gums. The procedure is not without irreversible sacrifice, but for the right patient, the protective return justifies the biological cost. The ultimate health outcome depends entirely on the precision of the clinician, the quality of the laboratory work, and the patient’s daily commitment to hygiene. When these align, veneers become a legitimate, lasting investment in the functional health of the mouth.
Frequently Asked Questions
Can I get a cavity under a veneer?
Yes. The porcelain itself cannot decay, but the natural tooth structure at the edge where the veneer meets the tooth is susceptible. If plaque accumulates at this margin and you do not clean it properly, acid will erode the tooth underneath, creating a cavity. Often, the cavity will progress significantly before you notice any dark line or change. Diligent flossing and regular dental checkups are essential to catch margin decay early.
Does getting veneers hurt?
The preparation process typically requires local anesthesia, so you should feel no pain during the procedure. The dentist removes a very thin layer of enamel, but that layer is not innervated. Some patients experience temporary cold sensitivity or gum soreness after the temporary veneers are placed or after the final bonding. This usually resolves within a few days. Lingering pain is not normal and should be evaluated immediately.
How long do the health benefits of veneers last?
When placed with excellent marginal adaptation and cared for meticulously, porcelain veneers can protect and serve you for 15 to 25 years or longer. The protective benefit persists as long as the veneer remains fully bonded, intact, and the margins stay sealed. If a margin opens, the protection is lost at that spot. This makes professional maintenance every six months critical to the longevity of the health benefit.
Do veneers make your breath smell?
Well-made, smooth veneers do not cause bad breath. In fact, by eliminating rough surfaces and food traps, they can reduce the bacterial load. However, if a margin is open, if there is cement residue left under the gum, or if you do not floss, the trapped bacteria will produce volatile sulfur compounds and cause halitosis. The restorations themselves are inert, but the environment around them must be kept pristine.
Will insurance cover veneers for health reasons?
Generally, dental insurance categorizes veneers as a cosmetic procedure and will not provide benefits. If you and your dentist can clearly document that the veneers are necessary to restore lost function, treat documented chronic pain, or rehabilitate a severely eroded dentition, you may have a case for partial coverage. This requires thorough pre-authorization with clinical notes, photos, and a narrative explaining the medical necessity. It is still rare, but worth pursuing in compelling functional cases.
Additional Resource
The American College of Prosthodontists offers an extensive patient education section detailing the science behind dental materials, tooth wear, and restorative options. You can find evidence-based guides on adhesive dentistry and the long-term management of tooth erosion at their official website: www.prosthodontics.org
Disclaimer: This article is intended for educational and informational purposes only and does not constitute medical or dental advice. It is not a substitute for a professional diagnosis or a personalized treatment plan. Always consult with a qualified dentist or prosthodontist regarding any questions about dental procedures, oral health conditions, or treatment options. Reliance on any information provided in this article is solely at your own risk.



