Do I Need Sinus Lift Surgery For a Dental Implant?
Losing a tooth is never part of the plan. One day, you are biting into an apple without a second thought. The next, you are staring at a gap in the mirror, wondering what happens now. Your dentist recommends a dental implant. You nod along, feeling relieved. Then they mention four words that change everything: sinus lift surgery. Your stomach drops. The term sounds terrifying, almost medieval. Questions flood your mind instantly. Is this really necessary? Can you avoid it? What does the procedure actually involve?
Take a deep breath. You are not alone in this moment of panic. Thousands of people face the exact same crossroads every year. The phrase “sinus lift” creates far more fear than it deserves. In reality, this procedure is one of the most predictable and well-documented bone grafting techniques in modern implant dentistry. It transforms impossible cases into successful smile restorations.
This guide will walk you through every aspect of sinus lift surgery. You will understand exactly what it is, why it matters, and how to determine if you genuinely need one. By the time you finish reading, the confusion will dissolve. You will have the clarity to make an informed decision about your oral health.
Understanding the Sinus Lift: What It Actually Means
Let’s strip away the medical jargon. A sinus lift is not as dramatic as it sounds. Surgeons do not literally “lift” your sinus like lifting a heavy box. The procedure is far more delicate and precise.
The Anatomy Behind the Procedure
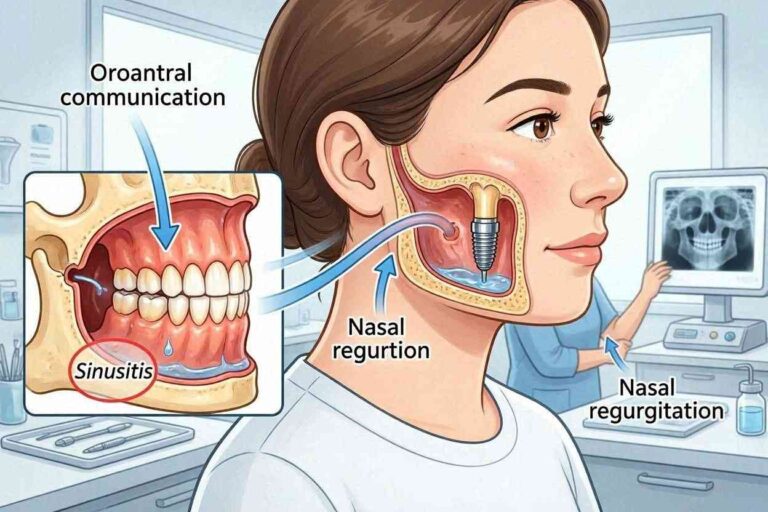
Your upper jaw sits directly beneath your maxillary sinuses. These are air-filled cavities located on either side of your nose. Think of them as empty rooms above your upper back teeth. Nature designed these spaces to lighten the weight of your skull, humidify the air you breathe, and influence the resonance of your voice.
Between these sinus cavities and your mouth lies a thin layer of bone. Dental implants need to anchor into this bone. The problem arises when there is not enough vertical height to support the implant fixture. An implant typically requires at least 8 to 10 millimeters of bone height to achieve long-term stability.
When a tooth in the upper jaw is lost and not replaced promptly, the body begins a natural process called resorption. The bone that once held the tooth root starts to dissolve away. The sinus cavity, sensing the empty space, often expands downward into the jawbone. This is a process called pneumatization. The result is a jawbone that is simply too thin to hold an implant securely.
Important Note: The sinus membrane is extremely thin and delicate. The “lift” in sinus lift surgery refers to the careful elevation of this membrane away from the jawbone. Once lifted, bone graft material is placed into the newly created space. Over several months, this graft transforms into your own living bone tissue, creating a solid foundation for the implant.
Why Bone Loss Happens in the Upper Jaw
To understand why you might need this procedure, you must grasp why upper jaw bone loss is so common. The posterior maxilla, or the back part of the upper jaw, has naturally less dense bone compared to the lower jaw. This is a simple fact of human anatomy. The bone is softer and more spongy.
When a molar or premolar is extracted, the healing process triggers a cascade of biological changes. The blood supply to the area decreases. The mechanical stimulation once provided by the tooth root disappears. The bone walls that held the tooth collapse inward. Within the first year after extraction, you can lose up to 25% of the bone width. Over several years, the vertical height also diminishes.
Simultaneously, the sinus cavity expands. The thin layer of bone separating the sinus from the mouth can become as thin as 1 or 2 millimeters. Placing an implant into this paper-thin bone would be like trying to hang a heavy picture on drywall without a stud. The implant would push through the sinus floor, penetrate the cavity, and likely fail. A sinus lift prevents this scenario entirely.
The Critical Connection Between Bone Density and Dental Implants
Dental implants are not natural teeth. They do not have a periodontal ligament that cushions forces. Instead, they achieve a mechanical lock with the bone through a process called osseointegration. This is the direct structural and functional connection between living bone and the surface of the implant.
Minimum Bone Requirements for Successful Implants
Osseointegration demands stability. The implant must sit rigidly in the bone during the healing phase. Any micromovement can cause a fibrous capsule to form around the implant instead of bone. This leads to failure.
The generally accepted minimum bone height for a standard diameter implant in the posterior maxilla is approximately 8 to 10 millimeters. The width should ideally be at least 6 millimeters. However, these numbers are not absolute. Surgeons consider the bone quality, your overall health, and the type of implant being used.
Here is a breakdown of how surgeons evaluate your bone:
| Bone Height Category | Measurement Range | Required Action for Implants |
|---|---|---|
| Adequate Bone | Greater than 10 mm | Standard implant placement is feasible without grafting. |
| Borderline Deficiency | 6 to 9 mm | Short implants may be possible, or a less invasive crestal sinus lift might be performed simultaneously with implant placement. |
| Severe Deficiency | Less than 6 mm | A lateral window sinus lift with bone grafting is typically required, often months before implant placement. |
What Happens When Bone Is Insufficient
Attempting to place an implant in severely deficient bone carries significant risks. The implant may perforate the sinus membrane. This creates an opening between the mouth and the sinus cavity, known as an oro-antral fistula. Saliva, bacteria, and food particles can then enter the sinus, causing chronic sinusitis.
Even if the membrane is not perforated, the implant will lack primary stability. It will feel wobbly to the surgeon. The long-term survival rate of an implant placed in inadequate bone is drastically lower. You could end up losing the implant within months or years, along with the money and time invested in the procedure. A sinus lift transforms a high-risk situation into a predictable one.
7 Clear Signs You Might Need a Sinus Lift
Now, let’s get specific. How do you know if this applies to you? Dentists do not recommend sinus lifts on a whim. They look for objective, measurable signs. Here are the seven most common indicators.
Sign 1: Long-Standing Tooth Loss in the Upper Back Jaw
Time is the enemy of jawbone. If you have been missing one or more upper molars or premolars for several years, the bone has likely undergone significant resorption. The body is extremely efficient. It redirects calcium and mineral resources away from areas that no longer serve a functional purpose. A missing tooth signals that the bone is no longer needed.
Even if you wore a partial denture, the pressure applied to the gum tissue does not replicate the internal stimulation of a tooth root. In fact, long-term denture wear can sometimes accelerate bone loss due to the compressive forces on the ridge. If your tooth has been gone for more than two years, a pre-implant CT scan will almost always reveal some degree of sinus proximity.
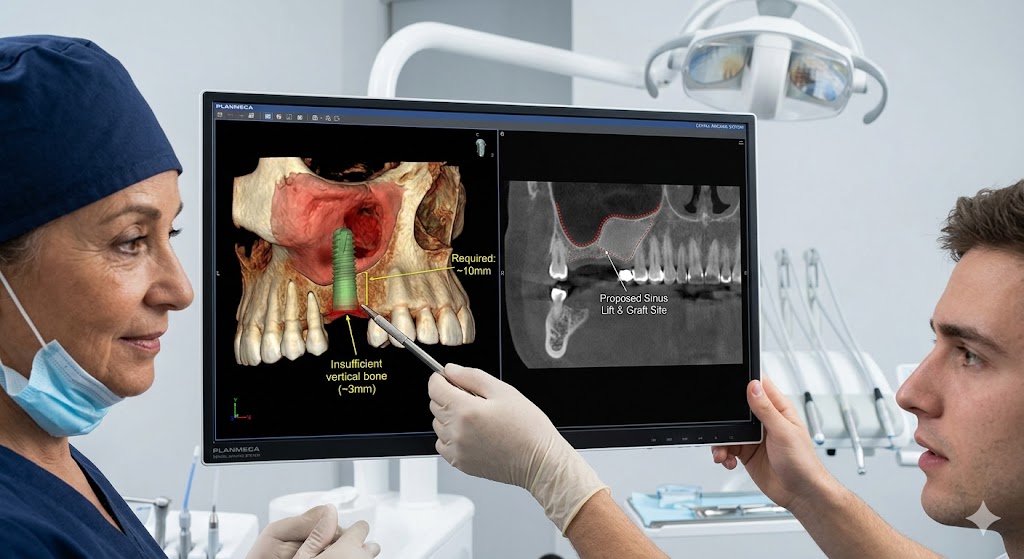
Sign 2: Your CBCT Scan Shows Limited Vertical Bone Height
The definitive diagnostic tool is a Cone Beam Computed Tomography scan. This is a three-dimensional X-ray that allows the surgeon to measure your bone with sub-millimeter accuracy. Unlike a traditional two-dimensional panoramic X-ray, a CBCT shows the exact three-dimensional anatomy of the sinus floor, the bone width, and the bone density.
During your consultation, the surgeon will scroll through the images on a screen. They will pinpoint the exact location of the sinus membrane and measure the distance from the ridge crest to the sinus floor. If this measurement falls below the required threshold, the scan provides the objective evidence you need a sinus lift.
Insight: A CBCT scan also reveals septa. These are bony walls or partitions within the sinus cavity itself. The presence of a septum can influence the surgical technique, making a lateral window approach more favorable than a crestal approach.
Sign 3: A Periodontal Disease History
Chronic gum disease does not just damage the soft tissue. The inflammatory process extends deep into the supporting bone. As periodontal bacteria accumulate, the body’s immune response activates cells called osteoclasts. These cells break down bone tissue. In advanced periodontitis, the bone loss can be extensive and rapid.
If you lost your upper back teeth due to gum disease, there is a high probability the bone was compromised long before the tooth was extracted. The infection often erodes the bone between the tooth roots and the sinus floor. Once the tooth is removed, you are left with a pre-existing bony defect that will not support an implant without augmentation.
Sign 4: A Large Sinus Cavity
Anatomy is a lottery. Some people are born with very low-sitting or large maxillary sinuses. This is a purely genetic trait. Even with perfectly healthy, present teeth, the sinus floor may extend far down between the tooth roots. Dentists can often see this on an X-ray: the roots of the upper molars appear to be tickling the sinus floor.
For these individuals, tooth loss almost guarantees a sinus lift will be necessary. There was minimal bone to begin with, and what little existed resorbs quickly. A person with naturally large sinuses has almost no margin for error when losing a back tooth.
Sign 5: Sinus Pneumatization Post-Extraction
As mentioned earlier, pneumatization is the expansion of the sinus cavity into the space left by missing teeth. It is a slow, natural phenomenon. The sinus does not recognize a boundary between itself and the jawbone. It simply grows to fill the void. This process can result in the sinus floor dipping down into the edentulous ridge, leaving virtually no bone for implant placement.
Sign 6: Previous Failed Implant in the Area
If you already attempted an implant and it failed, a sinus lift might be the solution. The failure may have been caused by unrecognized anatomical limitations. Perhaps the original implant was too short. Perhaps it perforated the sinus. The initial failure often results in some bone loss as well, making the situation worse. A sinus lift with grafting can reestablish the volume needed for a successful second attempt.
Sign 7: The Surgeon Recommends a Standard-Length Implant
Short implants exist. They are a viable option in some borderline cases. However, many surgeons prefer standard-length implants for their superior long-term data and biomechanical advantages. A standard implant (10 mm or longer) distributes chewing forces more favorably along its surface area. If your surgeon is committed to using a standard-length implant to achieve optimal crown-to-implant ratios, but your bone height is insufficient, a sinus lift becomes the biological requirement to accommodate that fixture.
Types of Sinus Lift Procedures: Which One Fits Your Case?
Not all sinus lifts are the same. The approach depends entirely on how much bone you have remaining. There are two primary techniques, with a third emerging option.
The Lateral Window Approach
This is the classic sinus lift procedure. Surgeons use it when the available bone height is severely deficient, typically less than 4 to 6 millimeters.
The procedure involves creating a small, oval-shaped window in the lateral wall of the maxilla. The surgeon accesses this area through the gum tissue on the cheek side of the jaw. Once the bone window is gently removed, the Schneiderian membrane—the lining of the sinus—becomes visible. Using specialized instruments, the surgeon carefully elevates this membrane from the bony floor of the sinus.
The membrane is extremely delicate, often compared to a wet tissue paper. A perforation is the most common intraoperative complication. If small, it can be repaired with a collagen membrane. If large, the procedure might need to be aborted and rescheduled after healing.
Once the membrane is elevated, the surgeon packs bone graft material into the newly created space. The bone window is often covered with a collagen membrane, and the gum tissue is sutured closed. Healing time typically ranges from 6 to 9 months before implant placement.
Key Point: The lateral window approach has a longer healing time and more postoperative swelling. However, it allows for a massive increase in bone height—often 10 to 15 millimeters—making it the only option for extremely atrophic ridges.
The Crestal (Osteotome) Approach
For borderline bone deficiencies, usually 6 to 9 millimeters of bone, a less invasive approach is possible. This is often called a crestal sinus lift, an osteotome lift, or a Summers lift.
Instead of creating a window in the side of the jaw, the surgeon prepares the implant site from the top of the ridge. They drill the initial hole for the implant, stopping 1 to 2 millimeters short of the sinus floor. Then, using instruments called osteotomes, they gently tap upward, fracturing the sinus floor in a controlled manner. This action elevates the sinus floor and the membrane locally, like an elevator going up a few floors. Bone graft material is often placed into the site before final elevation.
The significant advantage of the crestal approach is that implant placement can often happen simultaneously with the lift. Because the native bone is taller, the implant tip can engage the existing bone while the elevated area heals. This reduces treatment time dramatically. Recovery is also much less painful, with minimal bruising.
A Comparative Look at Your Options
This table summarizes the key differences between the two main approaches:
| Feature | Lateral Window Sinus Lift | Crestal (Osteotome) Sinus Lift |
|---|---|---|
| Ideal Bone Height | 1 to 5 mm of residual bone | 6 to 9 mm of residual bone |
| Surgical Access | Window created in the lateral jaw wall | Access directly through the implant site on the ridge crest |
| Membrane Visualization | Direct visualization of the sinus membrane | No direct visualization; relies on tactile feel |
| Simultaneous Implant | Rarely possible; implant placed 6-9 months later | Often possible during the same surgery |
| Postoperative Discomfort | Moderate swelling and bruising expected | Minimal discomfort, often comparable to a simple extraction |
| Primary Risk | Perforation of the sinus membrane | Disorientation of the osteotome, potential for uneven lifting |
Balloon Sinus Lift: A Modern, Less Invasive Option
A more recent development is the balloon sinus lift. This technique combines elements of both approaches but aims for minimal trauma.
The surgeon accesses the sinus floor through a very small crestal opening. A specialized balloon device is inserted and inflated with sterile saline. The gentle inflation pushes the membrane upward evenly and with less risk of tearing compared to manual instruments. Once the space is created, the balloon is deflated and removed, and bone graft is injected. This method is particularly useful when the sinus floor has a septa or an irregular anatomy that makes osteotomes risky.
Factors That Determine Candidacy: Beyond the X-Ray
A CBCT scan shows the anatomy, but it does not show the whole person. Several systemic and behavioral factors influence whether a sinus lift is suitable for you.
The Quality of Your Overall Health
Healing requires biological resources. Uncontrolled systemic conditions can severely compromise the outcome of a sinus lift. Diabetes, for instance, is not an absolute contraindication if it is well-managed. A hemoglobin A1c level below 7% is a commonly used benchmark. However, uncontrolled diabetes with high blood glucose impairs white blood cell function and new blood vessel formation, dramatically increasing the risk of graft failure and infection.
Autoimmune diseases, such as rheumatoid arthritis or lupus, may also interfere. More importantly, the medications used to treat these conditions, like corticosteroids or disease-modifying antirheumatic drugs, can suppress the immune system. Your dentist must consult with your rheumatologist to determine if a surgical pause in medication is safe.
Osteoporosis presents a nuanced picture. The condition itself reduces bone density, which is exactly what you are trying to rebuild. Bisphosphonate medications, particularly intravenous forms like zoledronic acid, carry a risk of medication-related osteonecrosis of the jaw. Oral bisphosphonates for osteoporosis carry a much lower risk, but your dental surgeon will still evaluate the duration of use.
Smoking and the Healing Conundrum
Smoking is one of the most significant modifiable risk factors in implant and grafting surgery. Nicotine is a potent vasoconstrictor. It narrows the tiny blood vessels that deliver oxygen and nutrients to the surgical site. Without robust blood flow, the graft material takes longer to revascularize.
Studies consistently show a higher failure rate for sinus grafts in smokers compared to non-smokers. Some surgeons will decline to perform the procedure unless the patient commits to a strict smoking cessation protocol for at least two weeks before and several months after surgery. The longer you can refrain, the better your odds of success.
Chronic Sinus Conditions
If you suffer from recurrent sinus infections, allergic rhinitis, or have a history of sinus surgery, the sinus lift procedure carries additional complexity. The Schneiderian membrane in these patients is often thickened, inflamed, or scarred. It may be more prone to tearing during elevation.
Active sinusitis is a temporary contraindication. The infection must be resolved with antibiotics or decongestants before proceeding. You do not want to introduce bacteria into a freshly placed bone graft. ENT consultation is often a valuable preoperative step for patients with complex sinus histories.
The Pre-Surgical Evaluation: What to Expect
You walk into the dental office for your sinus lift consultation. The path to a yes or no answer is methodical. Here is exactly what the process should look like.
The CBCT Scan: Seeing the Third Dimension
A standard panoramic X-ray flattens your anatomy into two dimensions. It cannot tell you the width of the bone. It cannot precisely identify the location of the sinus floor if it dips irregularly. The CBCT scan takes multiple images from different angles, reconstructing a 3D model of your skull.
The surgeon will sit with you and show you the cross-sectional slices. You will see the sinus as a black, air-filled space. You will see your jawbone as a grey structure. The critical measurement is the vertical distance from the top of the gum tissue ridge to the floor of the sinus. The software allows the surgeon to measure this exactly, eliminating guesswork.
Digital Implant Planning Software
Many modern practices go further. They import the CBCT data into specialized implant planning software. The surgeon can virtually place the implant on the screen, simulating the exact size, angle, and position. The software can superimpose a crown restoration, allowing for prosthetically driven planning. This ensures the implant will emerge in the optimal position to support the final tooth, not just where the bone is available. If the virtual placement fails due to insufficient bone, the software confirms the need for a sinus lift definitively.
Comprehensive Medical History Review
Expect a detailed questionnaire. The surgeon will ask about all current medications, including over-the-counter supplements. Aspirin, fish oil, vitamin E, and ginkgo biloba can thin the blood and should be paused before surgery. A history of bruising easily or bleeding for a long time after cuts will prompt a coagulation evaluation.
Allergies are critical. If you are allergic to penicillin, the surgeon will choose an alternative antibiotic. If you have a known allergy to certain bone graft materials, though rare, alternatives exist.
The Bone Graft Material: What Fills the Space
Lifting the membrane is only half the procedure. You need something to hold the membrane up while your body does the real work of regenerating bone. The choice of graft material is important.
Autografts: The Gold Standard
An autograft is bone harvested from your own body. For sinus lifts, the most common donor sites are the chin, the back of the lower jaw (ramus), or the tibia. The key advantage is biological. Autografts contain living osteoblasts, bone morphogenetic proteins, and growth factors. They provide a scaffold, and they also actively stimulate new bone formation. They are osteoinductive, osteoconductive, and osteogenic.
The downside is the need for a second surgical site. This means more postoperative discomfort and a slightly higher risk of complications like nerve damage or infection at the donor site.
Allografts and Xenografts: Reliable Alternatives
An allograft is human bone from a tissue bank. It undergoes rigorous processing to remove all cellular material and sterilize it. This eliminates the risk of disease transmission. Allografts are osteoconductive. They provide a scaffold onto which your own bone cells migrate and grow. They do not require a second surgical site, making recovery much more comfortable.
A xenograft is bone from an animal source, most commonly bovine (cow). The mineral structure of bovine bone is remarkably similar to human bone. Products like Bio-Oss are widely used and have decades of research supporting their safety and efficacy. The material is essentially a mineral matrix. It is very slowly resorbed by the body, providing long-term volume stability.
Synthetic Materials: The Alloplast
Alloplasts are man-made, such as beta-tricalcium phosphate or bioactive glasses. They eliminate any theoretical risk of biological contamination. Their resorption rates can be carefully engineered. Some formulations are designed to dissolve quickly as your bone replaces them. Others provide a permanent scaffold.
Quote from a Maxillofacial Surgeon: “The choice of graft material is not dogmatic. I tend to use a composite. Maybe 70% xenograft for long-term scaffold volume and 30% autograft from the implant preparation site to add those crucial growth factors. The best material is the one the surgeon is most experienced with and yields predictable results in their hands.”
A Step-by-Step Walkthrough of the Procedure
Understanding the sequence of events demystifies the surgery. Fear often stems from the unknown. Let’s walk through a typical lateral window sinus lift.
Before You Arrive
You will likely be prescribed a preoperative antibiotic. This establishes a blood level of the drug before the first incision, reducing the risk of surgical site infection. You will be told to have a light meal if you are having sedation, or to fast if undergoing general anesthesia. Arrange a driver. You will not be in a state to drive home.
The Day of Surgery: Anesthesia and Comfort
Sinus lift surgery is almost never performed with you completely unconscious unless combined with multiple other procedures. Most commonly, you will receive a combination of local anesthesia and conscious sedation. Oral sedation, like triazolam, or intravenous sedation with midazolam, will make you deeply relaxed. You will remain responsive but will remember little of the procedure afterward. The local anesthetic ensures zero pain during the surgery. The entire area, from the upper lip to the cheekbone, will feel numb and swollen.
The Incision and Access
Once you are comfortable, the surgeon makes an incision along the top of the gum ridge, slightly toward the palate. This placement allows for a good blood supply to the flap and ensures the final suture line will not sit directly over the bone window. The gum tissue is then gently elevated off the bone, exposing the lateral wall of the maxilla. This is the bone on the cheek side.
Creating the Window
Using a piezoelectric device or a surgical handpiece, the surgeon outlines a small oval or rectangular window. A piezoelectric device uses ultrasonic vibrations to cut bone without damaging soft tissue. This is crucial because the sinus membrane lies directly beneath the bone. The surgeon will cut until a thin layer of bone remains, or gently tap until the bone island is mobile. The bone window is then carefully teased away.
Elevating the Membrane
This is the most delicate phase. The surgeon uses specialized sinus curettes, which have angled, slightly cupped working ends. They slide the instrument between the bone floor and the membrane, gently lifting. You might hear a faint sound of scraping. You will feel pressure, but not pain. If the surgeon sees a tiny tear, they can often repair it by placing a collagen membrane over the defect. Once the membrane is elevated sufficiently, the tent-like space is ready for the graft.
Graft Placement and Closure
The bone graft material, often hydrated with saline or your own blood, is packed into the space. The surgeon fills the cavity until it is flush with the existing bone wall. A collagen membrane is often draped over the window site to prevent gum tissue cells from invading the graft. The gum tissue is then repositioned and sutured closed, usually with non-resorbable sutures that will be removed in one to two weeks.
Immediate Postoperative Period
You will go home with gauze in your mouth. Postoperative instructions are critical. You must not blow your nose for at least two to four weeks. The pressure can forcefully rupture the elevated membrane. You must sneeze with your mouth open to dissipate the pressure. You cannot drink through a straw. The suction can dislodge the clot and disrupt the graft.
Recovery Timeline: Healing Day by Day
Knowing what to expect after surgery reduces anxiety. Here is a realistic timeline.
The First 48 Hours
The initial 48 hours focus on managing bleeding and swelling. You will notice some pink-tinged saliva. This is normal. Some oozing from the nose, or even small graft particles appearing in your nose, is not uncommon. Apply ice packs to your cheek in 20-minute intervals. Sleep with your head elevated on two or three pillows. Stick to cold, soft foods. Take your prescribed pain medication before the local anesthetic wears off completely. The peak of swelling occurs around 48 to 72 hours.
Week One
Swelling begins to subside. Bruising often appears, migrating down your face. You might have a black eye. The bruising fades from purple to yellow to green, following gravity. You can begin warm saline rinses, but do not swish vigorously. Just tilt your head gently. You remain on a soft, non-chewing diet on the surgical side. Antibiotics continue until the bottle is empty. The sutures may start to feel irritating.
Weeks Two to Four
By two weeks, you are generally back to most normal activities, though heavy lifting and vigorous exercise are still restricted. Your sutures are removed around day 10 to 14. The gum tissue heals rapidly. Underneath the gum, the graft material is being infiltrated by blood vessels and stem cells. You must still refrain from blowing your nose. Air pressure differentials are the enemy during this phase. This means no flying in unpressurized aircraft, no scuba diving, and caution on very long commercial flights.
Months One to Six
The graft is consolidating. Your body is gradually replacing the graft material with your own woven bone. This process is called creeping substitution. You will have no sensation of this occurring. At a certain point, the surgeon will take a CBCT scan to assess the volume and density of the new bone. If sufficient, they can schedule the dental implant surgery. For a lateral window case, this typically happens around 6 to 9 months. For a crestal lift with simultaneous implant, the implant is already there, and you are waiting for osseointegration of the implant itself, which takes 3 to 4 months.
Weighing the Risks and Potential Complications
Honest conversations about risk empower you. Sinus lift surgery is highly successful, with success rates often cited above 95%. However, complications do occur.
Membrane Perforation
This is the most common intraoperative event, occurring in 10% to 25% of lateral window cases depending on the complexity of the anatomy. A small tear is usually inconsequential. The surgeon repairs it, the procedure continues, and the outcome is unaffected. A large perforation may require the surgeon to abort the procedure, as the graft material could dissipate into the sinus cavity. The membrane heals, and surgery can often be reattempted in a few months.
Postoperative Sinusitis and Infection
If the graft becomes infected, it will fail. Signs include persistent foul drainage from the nose, facial pain, fever, and a bad taste in the mouth. An infected sinus graft is a serious issue. Treatment involves antibiotics, and often, surgical debridement to remove the infected graft material. This is rare in healthy non-smokers, but the risk is real.
Graft Failure
Sometimes, the graft simply does not revascularize. It remains a mass of inert particles. The body encapsulates it in fibrous tissue instead of turning it into bone. When the surgeon returns to place the implant, they find a soft, gritty substance instead of solid bone. Risk factors include smoking, diabetes, and premature loading of the area.
Oro-Antral Communication
This is an opening between the mouth and the sinus. It creates a pathway for fluids. Small communications can heal spontaneously with careful management and antibiotics. Larger ones require a second surgical procedure to close the defect with a buccal fat pad advancement or a palatal flap.
The Cost Landscape: Investing in Your Health
The price of a sinus lift varies widely based on geographic location, surgeon expertise, and graft material used. Here is a general breakdown of costs in the current market.
Fee Itemization
- Consultation and CBCT Scan: $200 to $600. This is often credited toward the procedure if you proceed.
- Lateral Window Sinus Lift (one side): $2,500 to $6,000. This fee typically includes the surgeon’s time, facility fee, anesthesia, bone graft material, and membrane.
- Crestal Sinus Lift (one side): $1,500 to $3,500. Less time and material mean lower cost.
- Dental Implant (post-grafting): $1,500 to $3,000 for the fixture.
- Implant Crown: $1,500 to $3,000.
A Cost Comparison Table
This table gives you a realistic view of the total investment for a single tooth replacement in the posterior maxilla.
| Treatment Pathway | Procedure Costs (Estimated) | Total Timeline |
|---|---|---|
| Pathway 1: No Graft Needed | Implant + Crown: $3,000 – $6,000 | 3 – 6 months |
| Pathway 2: Crestal Lift + Immediate Implant | Crestal Lift + Implant + Crown: $5,000 – $9,500 | 4 – 7 months |
| Pathway 3: Lateral Window Lift + Delayed Implant | Lateral Lift (wait 6-9 mo) + Implant + Crown: $7,000 – $12,000 | 9 – 15 months |
| Alternative: Tooth-Supported Bridge | 3-Unit Bridge: $3,500 – $5,000 | 2 – 4 weeks |
| Alternative: No Treatment | Progressive bone loss, potential sinus issues, shifting teeth | Lifetime |
Insurance and Financing
Dental insurance often considers the implant and crown a major restorative procedure. Coverage varies. The sinus lift itself is often coded as a surgical procedure, sometimes falling under medical insurance if sinus pathology or trauma is involved. Ask for a pre-treatment estimate. Most offices offer third-party financing plans, like CareCredit, that break the total fee into manageable monthly payments.
Alternatives to Sinus Lift Surgery
Is there any way around it? In some specific situations, yes. You should explore all options.
Short Dental Implants
Short implants are typically 6 to 8 millimeters in length. They have been developed specifically for atrophic ridges. Their surface technology is more advanced, with highly roughened surfaces to maximize bone-to-implant contact in a limited height.
If you have between 5 and 8 millimeters of bone, a short implant with a wide diameter might be feasible without a sinus lift. Long-term studies show very high survival rates, comparable to standard implants. However, biomechanically, a short implant has a less favorable crown-to-implant ratio. The crown is often longer than the implant, creating a lever effect. The restoration must be meticulously designed to avoid excessive lateral forces.
Zygomatic Implants
For the most extreme cases, where the maxillary bone is completely resorbed, there is a dramatic solution: the zygomatic implant. This is a very long implant, usually 30 to 50 millimeters, that is anchored not in the jawbone, but in the zygomatic bone—your cheekbone.
This procedure is complex and carries significant risks, including potential nerve damage and orbital complications. It is almost always performed under general anesthesia by a highly specialized maxillofacial surgeon. It avoids the need for a sinus lift and multiple bone grafts entirely. However, it is reserved for patients with severe maxillary atrophy who do not want removable dentures.
Traditional Bridges and Dentures
Returning to the non-implant options, a tooth-supported bridge is a viable path. It requires the teeth on either side of the gap to be prepared for crowns. The bridge spans the gap with a false tooth. It requires no bone grafting. However, it sacrifices healthy tooth structure and does not prevent the bone loss in the empty site.
A removable partial denture is the least expensive option. It rests on the gums and clasps onto other teeth. It does not stop bone resorption. In fact, it often accelerates it. But for patients who are medically or financially unable to pursue grafting and implants, it restores some chewing function and aesthetics.
How to Discuss This with Your Dental Team
You are now armed with knowledge. As you sit back in the dental chair, you can be an active participant in the conversation. Do not hesitate to ask specific questions.
Questions to Ask Your Surgeon
- “Can I see my CBCT scan? Will you show me the exact measurement from the ridge to the sinus floor?”
- “Based on my scan, are you recommending a lateral window or a crestal approach? Why?”
- “What type of bone graft material do you prefer for a case like mine, and what is your success rate with it?”
- “What is your protocol for managing a membrane perforation if it occurs?”
- “Are you placing the implant the same day, or do I need to wait? If waiting, how many months?”
- “What are the absolute do-nots for my recovery, specifically regarding nose blowing and flying?”
Understanding Informed Consent
Informed consent is not just a signature on a form. It is a process. Your surgeon should explain the nature of your condition, the proposed procedure, the material risks, the benefits, and the alternatives, including no treatment. If you feel rushed or your questions are dismissed, seek a second opinion. A genuine professional welcomes a patient who takes an active interest in their care.
Conclusion
A sinus lift is not an optional extra; it is the biological foundation for a successful upper jaw dental implant when bone height is insufficient. By gently raising the sinus membrane and placing bone graft material, this procedure creates the solid base necessary to support osseointegration and prevent implant failure. Though the term sounds intimidating, the surgery is precise and highly predictable, with most patients returning to normal function quickly. The decision ultimately rests on a three-dimensional CBCT scan, your health status, and a transparent conversation with a skilled surgical team, empowering you to move from tooth loss anxiety toward a lasting, confident smile.
Frequently Asked Questions
How painful is sinus lift surgery?
Most patients are surprised by the limited nature of the pain. The procedure is performed under local anesthesia with sedation, so you feel no pain during surgery. Postoperatively, you can expect manageable discomfort, similar to a sinus headache or pressure, typically well-controlled with prescribed analgesics. The swelling and bruising are often more bothersome than the pain itself.
Can a sinus lift be avoided if I get an implant immediately after an extraction?
Potentially, yes. A procedure called alveolar ridge preservation involves placing bone graft into the socket immediately after tooth removal. This slows the resorption and pneumatization process. If the existing bone is already tall, this can prevent the need for a future sinus lift. However, if your sinus floor is inherently low, ridge preservation alone may not provide the necessary vertical height.
Will my voice change after a sinus lift?
No significant permanent change occurs. The sinus cavity volume is reduced slightly by the elevation of the floor, but this does not alter the resonant frequency of your voice in a noticeable way. If you are a professional opera singer or voice actor, discuss this with your surgeon, but for the general population, no one will know you had the procedure from your voice.
Is a sinus lift covered by medical or dental insurance?
It is often a grey area. The sinus lift is a surgical procedure that may be billed to medical insurance, especially if there is a reconstructive or functional component. However, many medical insurers classify it as dental. Dental insurance may cover a portion under oral surgery benefits. You must work with the office to obtain a pre-treatment estimate to know your exact financial responsibility.
Disclaimer:
This article is for informational and educational purposes only and does not constitute medical or dental advice. The content is not intended to be a substitute for professional diagnosis, treatment, or guidance from a licensed dentist or physician. Always seek the advice of your qualified healthcare provider with any questions you may have regarding a medical condition or treatment.