most common cause of dental implant failure
So, you have invested time, money, and hope into a dental implant. Or perhaps you are considering getting one. Either way, the question lurking in the back of your mind is a valid one: What if it fails?
Let’s be honest with each other. Dental implants are one of the greatest successes in modern dentistry. They boast success rates above 95% over ten years. But nothing in medicine is perfect. Failures happen.
Understanding why they fail is your best protection. And here is the truth that many people find surprising: The most common cause of dental implant failure is not an accident, a bad fall, or even poor bone quality. It is a bacterial infection called peri-implantitis.
This article will walk you through exactly what that means, why it happens, and—most importantly—how to prevent it. No fluff. No fake promises. Just the reliable guide you need.
What We Mean by “Implant Failure”
Before we talk about causes, we need a clear definition. When dentists say an implant has failed, they usually mean one of two things.
Early Failure vs. Late Failure
| Type of Failure | Timeframe | Main Characteristics |
|---|---|---|
| Early Failure | First 3–6 months (before crown is placed) | The implant never bonds with the bone. It remains loose or gets rejected. |
| Late Failure | After 1 year or more | The implant worked initially, but problems develop later. Usually infection-related. |
Early failures are often linked to surgical technique or healing issues. Late failures are almost always linked to the most common cause we are discussing today.
Important Note: Not every pain or problem is a failure. Some issues like screw loosening or gum irritation can be fixed without removing the implant. True failure means the implant must be surgically removed.
The Number One Culprit: Peri-Implantitis
If you remember only one word from this entire article, let it be peri-implantitis.
Think of it as a cousin to gum disease. But a more aggressive one.
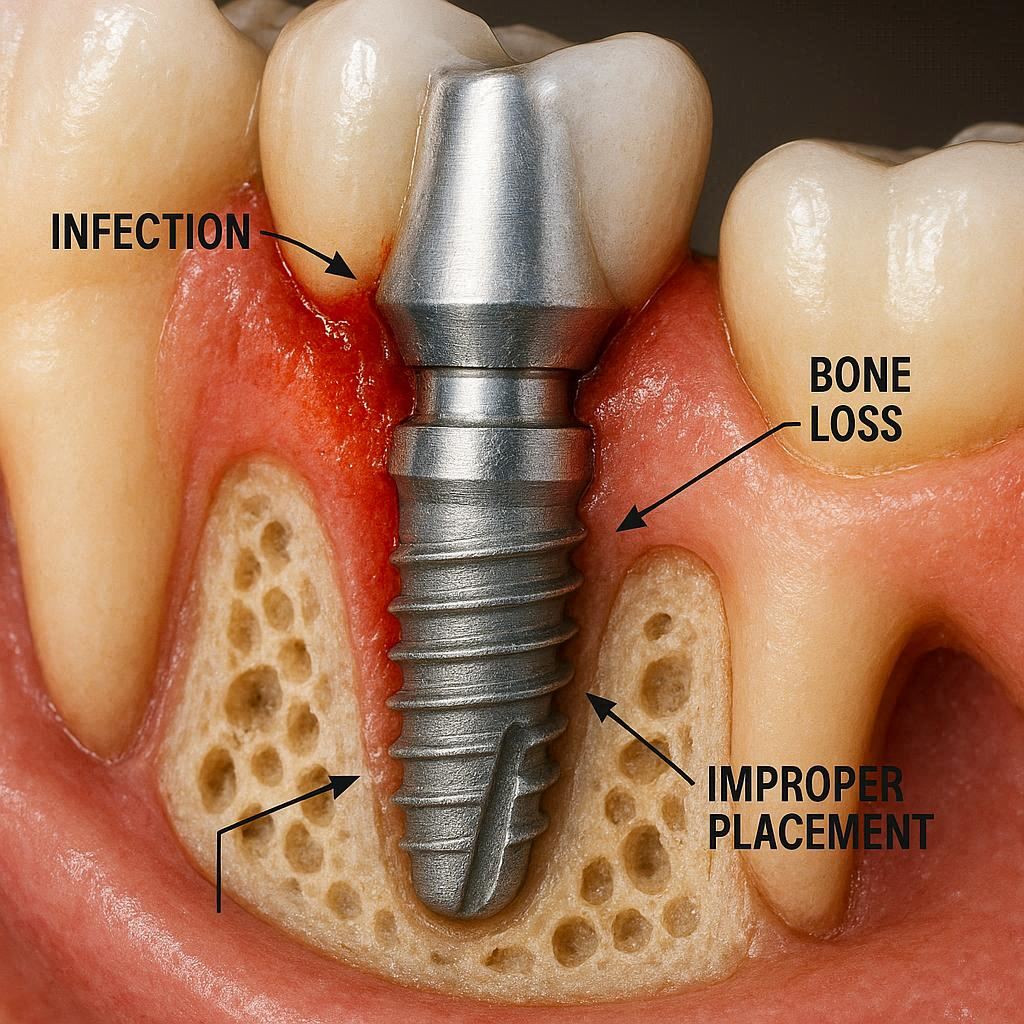
Peri-implantitis is a destructive inflammatory process. It affects the soft and hard tissues surrounding a dental implant. It causes:
- Inflammation of the gums (swelling, redness, bleeding)
- Loss of supporting bone (the bone literally melts away around the implant threads)
- Progressive pocketing (deep gaps form between the gum and the implant)
When peri-implantitis is left untreated, it destroys the bone that holds the implant in place. The implant becomes mobile. Eventually, it falls out or must be removed.
How Peri-Implantitis Starts
It almost always begins with a simpler condition called mucositis.
Mucositis is a reversible gum inflammation around the implant. Imagine it as a warning light on your car dashboard. If you ignore it, the engine overheats. In this case, ignoring mucositis allows bacteria to travel deeper, reaching the bone.
Once the bacteria invade the bone-implant interface, mucositis turns into peri-implantitis. And that is where the real trouble begins.
Why Is Peri-Implantitis So Common?
Unlike a natural tooth, a dental implant has no periodontal ligament. That ligament acts as a shock absorber and a barrier against bacteria in natural teeth. Implants have a direct bone-to-implant contact. That connection is strong, but it is also vulnerable.
Bacteria can sneak into the microscopic gaps between the implant and the abutment (the connector piece). They form a biofilm. Your body’s immune system fights back, but in doing so, it also destroys its own bone tissue. That is the cruel paradox of peri-implantitis.
Other Common Causes (But Not the Most Common)
Let’s be fair. Peri-implantitis is the leader, but it is not the only cause. Here are other reasons why implants fail. Understanding this list gives you the full picture.
1. Failed Osseointegration (Early Failure)
Osseointegration is the fancy term for “bone bonding.” For an implant to succeed, your jawbone must grow tightly around the titanium surface. If that process fails, the implant never stabilizes.
Why does osseointegration fail?
- Overheating the bone during drilling (surgical error)
- Contamination of the implant surface (during handling)
- Premature loading (putting a crown on before the bone is ready)
- Poor bone quality or quantity (very soft or very dense bone)
2. Medical Conditions and Medication
Your overall health plays a massive role.
| Condition / Medication | Impact on Implants |
|---|---|
| Uncontrolled diabetes | Slows healing, increases infection risk |
| Osteoporosis medications (bisphosphonates) | Risk of osteonecrosis (bone death) |
| Autoimmune diseases | Chronic inflammation disrupts healing |
| Heavy smoking | Reduces blood flow, impairs bone healing |
3. Surgical Trauma
Even the best surgeon can face surprises. But certain surgical mistakes increase failure risk:
- Nerve damage (leading to chronic pain or numbness)
- Perforation of the sinus cavity (for upper implants)
- Using an implant that is too small or too large for the bone ridge
4. Parafunctional Habits (Grinding and Clenching)
Bruxism—the medical name for teeth grinding—is a silent killer of implants.
Why? Because an implant has no shock absorber. Every time you clench or grind, you transfer extreme force directly to the bone. Over time, this can:
- Crack the implant body
- Loosen the abutment screw
- Fracture the crown
- Cause bone microfractures that lead to failure
5. Allergic Reaction to Titanium
This is extremely rare. Less than 1% of patients have a true titanium allergy. But it exists. Symptoms include chronic inflammation, rashes, and persistent pain with no other explanation.
Risk Factors You Can Control vs. Those You Cannot
Let’s organize this information in a way that empowers you.
Risk Factors You CANNOT Change
- Your genetics (family history of gum disease)
- Previous radiation to the jaw (for cancer treatment)
- Severe bone loss from birth defects or old trauma
- Certain autoimmune conditions
Risk Factors You CAN Change or Manage
- Your daily oral hygiene (game changer)
- Smoking or vaping (single biggest modifiable risk)
- Blood sugar control (if diabetic)
- Regular professional maintenance (every 3–6 months)
- Avoiding hard foods on the implant crown
- Wearing a nightguard if you grind your teeth
Realistic truth: You can have multiple risk factors and still succeed. But you need to be honest with your dentist and yourself. Implants are not magic. They work with you, not despite you.
Early Warning Signs: How to Know Trouble Is Coming
The best way to stop the most common cause of failure is to catch it early. Here is what you should watch for.
In the First Month After Surgery (Early)
- Increasing pain after the first week (should improve, not worsen)
- Movement of the implant (gently test with your tongue)
- Pus or foul discharge from the gum around the implant
- Fever or swelling spreading to your face or neck
What to do: Call your surgeon immediately. Do not wait.
After the Crown Is Placed (Late Signs of Peri-Implantitis)
These are the signs most people ignore until it is too late.
- Bleeding when brushing around that specific implant
- Bad taste in your mouth that does not go away
- Gums that look red and puffy (not pink and firm)
- Receding gums exposing the implant threads
- Deep pockets when your dentist probes (anything over 5mm)
- Loose crown (the tooth feels wiggly)
Quote from a periodontist (paraphrased for clarity):
“Patients often tell me, ‘It doesn’t hurt, so it must be fine.’ That is a dangerous myth. Peri-implantitis is often painless until the very end stage. By the time you feel pain, you have likely lost significant bone.”
Diagnosis: How Dentists Confirm the Problem
Your dentist has tools you do not. Here is what they look for.
- Probing depths: A tiny ruler measures the gum pocket around your implant. Healthy is 2–3mm. Problematic is 5mm or more.
- Bleeding on probing: If the gum bleeds easily, inflammation is active.
- X-rays (radiographs): These show bone levels. Your dentist compares current X-rays to the ones taken right after placement. Bone loss means failure is progressing.
- Mobility testing: If the implant moves, the bone-implant bond is broken. That is a failed implant.
Treatment Options: Can a Failing Implant Be Saved?
Yes, sometimes. But honesty is crucial.
For Peri-Implantitis (Early to Moderate)
If detected early, you have options.
| Treatment | What It Does | Success Rate |
|---|---|---|
| Non-surgical debridement | Deep cleaning with special plastic instruments (metal scratches titanium) | Good for early mucositis |
| Laser therapy | Kills bacteria and removes inflamed tissue | Moderate |
| Open flap debridement | Surgery to lift the gum and clean the implant surface | Better for moderate bone loss |
| Bone grafting | Adds bone to the area, but success is unpredictable around infected implants | Variable |
When Removal Is the Only Option
Sometimes, the implant is beyond saving. Signs it is time to remove:
- Bone loss greater than 50% of the implant length
- Mobility (implant moves)
- Persistent pus and infection despite treatment
- Patient refuses to change hygiene or smoking habits
Here is the silver lining: After removal, the bone usually heals in 3–6 months. You can often try a new implant in the same spot. Many people succeed the second time.
Prevention: Your Best Weapon
Let’s focus on what really matters. You want to avoid the most common cause of dental implant failure. Here is your practical checklist.
Daily Home Care (Non-Negotiable)
Natural teeth are easy. Implants are not. You need specific tools.
Your implant hygiene kit should include:
- Soft-bristle toothbrush (ultrasoft is better)
- Interdental brushes (small brushes that fit between teeth)
- Water flosser (like Waterpik with a special implant tip)
- Plastic or titanium scalers (never metal from a drugstore)
- Low-abrasive toothpaste (avoid baking soda or charcoal)
Daily routine:
- Brush twice a day, paying special attention to the gumline around the implant.
- Use a water flosser on low pressure. Aim the tip at a 45-degree angle toward the gum.
- Clean between the implant crown and adjacent teeth with interdental brushes.
- Rinse with an alcohol-free, antibacterial mouthwash (your dentist can recommend one).
Professional Maintenance Schedule
Do not skip your checkups. Seriously. This is where most patients fail.
| Risk Level | Recommended Maintenance Visits |
|---|---|
| Low risk (non-smoker, good health, good hygiene) | Every 6 months |
| Moderate risk (former smoker, well-controlled diabetes) | Every 4 months |
| High risk (current smoker, poor hygiene, history of gum disease) | Every 3 months |
At each visit, your dentist or hygienist should:
- Measure probing depths around every implant
- Take periodic X-rays (usually yearly)
- Clean with implant-safe instruments (plastic or graphite)
Lifestyle Modifications
I will not lecture you. But I will give you the unvarnished truth.
- Smoking: If you smoke, your implant failure rate is roughly double to triple that of a non-smoker. Vaping is not safe either. The nicotine constricts blood vessels. Less blood flow means less healing.
- Diabetes: Keep your HbA1c below 7.0% before surgery. High blood sugar feeds bacteria and impairs white blood cells.
- Grinding: Get a custom nightguard. Not a drugstore boil-and-bite. A custom one from your dentist. It costs $300–$600. Compare that to $4,000–$6,000 for a new implant.
Debunking Common Myths
Let’s clear up some misinformation floating around the internet.
Myth 1: “Implants last forever.”
Truth: With perfect care, they can last 20, 30, or even 40 years. But “forever” is not realistic. The crown on top will wear out. The implant can still fail if neglected.
Myth 2: “If my implant fails, it is always the dentist’s fault.”
Truth: Sometimes it is. Surgical errors happen. But the vast majority of late failures are patient-related. Poor hygiene, smoking, and skipping maintenance are patient choices.
Myth 3: “I have gum disease, so I cannot get implants.”
Truth: You must control the gum disease first. Once it is stable, implants can succeed. Many periodontists place implants in patients with a history of gum disease, with good success, as long as the patient commits to rigorous maintenance.
Myth 4: “Titanium implants cause cancer.”
Truth: No credible scientific evidence supports this. Titanium is biocompatible and used in hip replacements, knee replacements, and dental implants for decades.
What the Research Says (Simple Version)
For those who like data, here is the short version of what scientific studies tell us.
- A large systematic review (over 10,000 implants) found that peri-implantitis affects between 18% and 28% of patients over 10 years.
- That means roughly 1 in 4 to 1 in 5 implant patients will develop this condition.
- Smokers have a 140% higher risk of implant failure compared to non-smokers.
- Diabetes increases failure risk by approximately 50% when poorly controlled.
- Good oral hygiene reduces the risk of peri-implantitis by over 70%.
My take as a writer: Those numbers are not scary. They are informative. Knowing the risk means you can take action.
Special Cases Worth Discussing
Immediate Load Implants (Teeth in a Day)
These are implants where the dentist places a temporary crown immediately after surgery. They are convenient, but they have a slightly higher early failure rate because the bone is healing under pressure.
Verdict: For the right candidate, they work. But if you have any risk factors (smoking, grinding, soft bone), traditional two-stage implants are safer.
Zirconia Implants (Metal-Free)
Some patients choose zirconia because they fear metal allergies or prefer a white color. Zirconia is less flexible than titanium and can fracture under extreme force.
Failure cause: Fracture of the implant body, not peri-implantitis (zirconia is more resistant to bacterial colonization but less resistant to mechanical stress).
All-on-4 or All-on-6 (Full Arch)
These are full sets of teeth supported by four or six implants. They are revolutionary. But they are also high-maintenance.
Special risk: Keeping the area under the bridge clean is difficult. Food traps easily. Without daily use of superfloss and water flossers, peri-implantitis develops rapidly.
How to Choose a Dentist to Minimize Failure Risk
You cannot control everything. But you can choose a skilled professional. Here is a checklist.
- Ask about their implant training: General dentists can place implants. But oral surgeons and periodontists have 3+ extra years of surgical training.
- Ask about surgical guides: Do they use 3D planning and computer-guided surgery? This reduces error.
- Ask about their failure rate: A good dentist will be honest. An average rate is 3–5% over 5 years.
- Ask about maintenance protocols: If their office does not have a dedicated implant maintenance program, keep looking.
Red flags:
- Guarantees of 100% success
- Pushing you to rush treatment
- No discussion of your medical history
- No X-rays taken during consultation
Real-Life Scenarios: How Failure Happens Step by Step
Let me paint you a picture. Perhaps it will sound familiar.
Scenario A: The Busy Professional
Sarah, 45, gets a single implant for a missing molar. She is a non-smoker and healthy. She follows post-op instructions perfectly. For two years, everything is fine.
Then life gets busy. She stops flossing around the implant because it is “hard to reach.” She skips her annual checkup for three years. Eventually, she notices bleeding when brushing. She ignores it. Six months later, the implant feels slightly loose.
Her dentist takes an X-ray. The bone loss is severe. The implant cannot be saved.
Cause: Neglected peri-implantitis that started as simple mucositis. Preventable.
Scenario B: The Optimistic Grinder
Mark, 55, gets two implants in his lower jaw. He grinds his teeth at night but never told his dentist. The implants heal fine. The crowns are placed.
Mark does not wear a nightguard because he “does not like the feeling.” Within 18 months, one crown cracks. Then the other implant starts feeling sore.
Upon examination, both implants show bone loss and one implant body is fractured.
Cause: Biomechanical overload from bruxism, combined with late peri-implantitis.
What to Do If Your Implant Is Already Failing
If you are reading this and worried your implant is failing, do not panic. Follow these steps.
- Stop home remedies. Do not poke, prod, or use undiluted essential oils. You can make it worse.
- Call your dentist tomorrow. Do not wait weeks. Time equals bone.
- Gather your records. Find your implant surgery date, implant brand (if known), and any X-rays.
- Ask for a referral if your general dentist seems unsure. A periodontist is your best resource for failing implants.
- Be ready for a tough conversation. You may need to remove the implant. That is not a failure of you as a person. It is a medical reality. Many people try again successfully.
Cost Considerations
Let’s talk money. Because it matters.
| Procedure | Estimated Cost (USA, without insurance) |
|---|---|
| Single implant + crown | $3,000 – $6,000 |
| Implant removal | $500 – $1,500 |
| Bone grafting (after removal) | $800 – $2,500 |
| New implant + crown | $3,000 – $6,000 (again) |
| Peri-implantitis treatment (non-surgical) | $300 – $800 |
| Peri-implantitis surgery (open flap) | $1,500 – $4,000 |
Financial tip: Some dental insurance plans cover implant removal and treatment of infections (peri-implantitis) even if they do not cover the implant placement itself. Check your policy.
The Emotional Side of Implant Failure
We talk about bone, bacteria, and budgets. But we rarely talk about how it feels.
Failed implants can cause:
- Frustration because you spent thousands of dollars
- Embarrassment because you blame yourself
- Fear of trying again
- Anger at your dentist or yourself
All of these feelings are normal. But here is what I want you to remember:
A failed implant is a biological event, not a moral failure.
Good people with excellent hygiene still have peri-implantitis. Bodies are unpredictable. The most important thing is to learn from the experience, treat the problem, and decide if you want to try again with a better plan.
Summary Table: Main Causes at a Glance
| Cause | Percentage of Failures (Approx.) | Preventable? |
|---|---|---|
| Peri-implantitis (infection) | 40–60% | Yes, with hygiene + maintenance |
| Failed osseointegration (early) | 10–20% | Partially (depends on surgeon + bone quality) |
| Biomechanical overload (grinding) | 10–15% | Yes (nightguard) |
| Medical conditions | 10–15% | Partially (manage underlying disease) |
| Surgical error | 5–10% | Yes (choose an experienced surgeon) |
| Other (allergy, fracture, etc.) | <5% | Rarely |
Conclusion (Three Lines)
The most common cause of dental implant failure is peri-implantitis—a bacterial infection that destroys the bone holding the implant. You can prevent it through meticulous daily cleaning, avoiding smoking, and never skipping professional maintenance visits. If you catch the warning signs early (bleeding gums, bad taste, pocketing), many failing implants can be saved before removal becomes necessary.
Frequently Asked Questions (FAQ)
1. Can a failed dental implant be replaced?
Yes. After the failed implant is removed, the bone usually heals in 3–6 months. In many cases, a new implant can be placed in the same location.
2. How do I know if my implant is failing?
Look for mobility (wiggliness), bleeding when brushing around that specific tooth, persistent bad taste, pus, or visible gum recession exposing metal threads.
3. Is peri-implantitis painful?
Not usually in the early stages. It is often painless until significant bone loss has already occurred. That is why regular dental checkups are essential.
4. Can antibiotics cure peri-implantitis?
No. Antibiotics can suppress the infection temporarily, but they cannot remove the bacterial biofilm from the rough implant surface. Physical cleaning (by a dentist) is required.
5. What is the most common cause of early implant failure (first 3 months)?
Failed osseointegration (the bone never bonds to the implant). This is often related to surgical technique, infection at the time of surgery, or patient factors like uncontrolled diabetes.
6. Are zirconia implants less likely to fail from infection?
Some studies suggest zirconia accumulates less plaque than titanium. However, zirconia is more brittle and can fracture under grinding forces. Neither material is failure-proof.
7. How long do dental implants typically last?
With excellent care, 20+ years is common. The crown may need replacement after 10–15 years, but the implant itself can last a lifetime if peri-implantitis is prevented.
8. Can I get an implant if I have gum disease?
Yes, but only after the gum disease is treated and stabilized. Active gum disease near an implant will rapidly progress to peri-implantitis.
Additional Resource
For a deeper, evidence-based look at peri-implantitis prevention, visit the American Academy of Periodontology’s patient page on implant maintenance. They offer downloadable guides and checklists for patients.
👉 AAP.org/patients/peri-implantitis (Note: This is for reference. Always consult your own dentist for personalized advice.)



