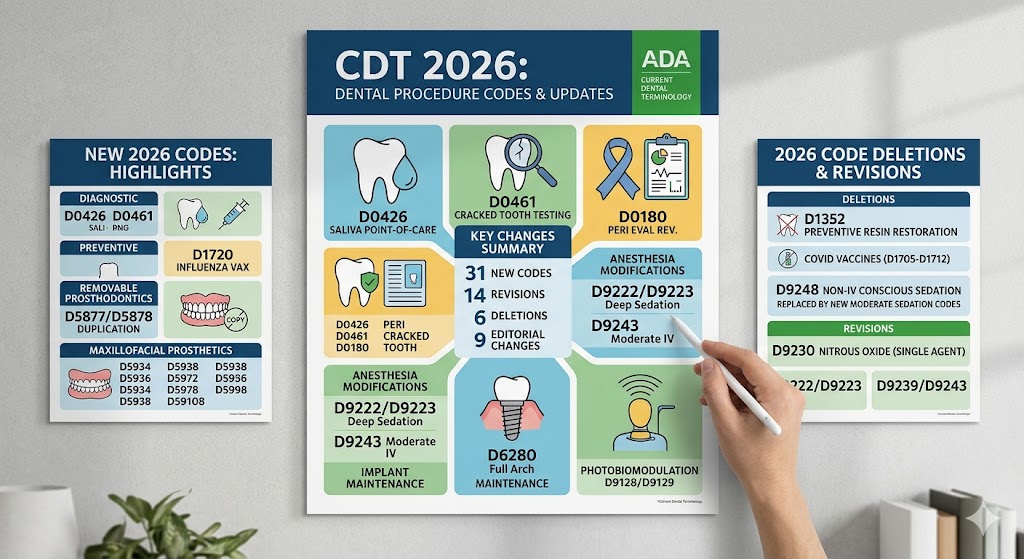
Dental Codes for Procedures 2026
Accuracy in dental billing feels like a moving target. Just when your front desk team masters the current year’s codes, a new cycle approaches. The transition to 2026 brings a fresh set of Current Dental Terminology (CDT) codes, and staying ahead protects your revenue cycle.
This guide walks you through every significant change effective January 1, 2026. You will find practical explanations, clinical scenarios, and billing strategies. We focus on what matters most: clean claims, compliant documentation, and a stress-free billing department.
Important Note: The American Dental Association (ADA) maintains strict control over the CDT manual. The codes discussed here align with the official release timeline. This article reflects the standard annual update process and serves as an educational resource only. Always verify codes directly with the ADA’s official publication or your practice management software update before submitting claims.
Understanding the CDT Code Maintenance Cycle
The ADA’s Code Maintenance Committee (CMC) manages an ongoing cycle of updates. Understanding this rhythm helps your practice prepare rather than react.
The Annual Timeline
The CMC accepts requests for new codes, revisions, and deletions each year. Submissions undergo rigorous review. The committee votes during a public meeting, typically held in the spring. Approved changes then take effect the following January 1. For the 2026 update, the key votes occurred in March 2025.
You receive the final code set through multiple channels. The ADA publishes the physical CDT manual in the fall. Practice management software vendors push electronic updates in late December. Many payers require a brief implementation period before fully recognizing new codes.
Why Codes Change
Codes evolve for three primary reasons. First, technology advances faster than the code set. New procedures require unique identifiers. Second, third-party payers demand greater specificity for utilization review. Third, clinical practice patterns shift, rendering older codes obsolete or overly broad.
A procedure you performed frequently in 2023 may now require a different documentation standard or a completely separate code. The 2026 update emphasizes precision in implant therapy, digital workflows, and therapeutic treatments for sleep-disordered breathing.
Key Themes Defining the 2026 Update
Several major trends shape this year’s changes. Recognizing these patterns simplifies learning the individual codes.
The Digital Impasse Resolved
For years, clinicians struggled to code digital impressions and same-day restorations accurately. The indirect pulp cap code didn’t quite fit an optical scan. The prefabricated crown code didn’t capture the design work of a chairside milled restoration. The 2026 update introduces dedicated pathways for fully digital workflows, finally separating the acquisition of data from the physical restoration.
Implant Maintenance Matures
Implant dentistry codes previously focused heavily on surgical placement and prosthetic components. Long-term maintenance received less granular attention. The 2026 code set addresses peri-implantitis treatment, implant removal due to biological failure, and sophisticated prosthetic repairs. This signals payer recognition that implant complications require distinct, billable interventions.
Medical-Dental Integration Deepens
Sleep apnea appliances now have codes that better align with medical payer requirements. Pharmacologic management codes also receive attention, particularly agents applied for caries arrest. This crossover reflects a broader industry push toward valuing oral health’s impact on systemic conditions.
Comprehensive Breakdown of 2026 CDT Codes by Category
Let’s move through the code families most impacted this year. Each section explains the clinical context and documentation requirements.
Diagnostic Procedures (D0100-D0999)
Diagnostic coding sees modest but meaningful refinements. The goal remains capturing the level of clinical decision-making involved in assessment.
D0150: Comprehensive Oral Evaluation – New Patient
No change to the code number itself, but the 2026 manual descriptor now explicitly includes a statement regarding the optional integration of a digital caries susceptibility assessment. If you use fluorescence-based or transillumination-based detection as part of the comprehensive exam, document the findings. The exam’s core remains the same, but the descriptor validates your technology use.
D0251: Extra-Oral Posterior Dental Imaging
This code once referred narrowly to specific temporomandibular joint projections. The revised nomenclature accommodates newer extra-oral imaging units that capture posterior periapical-like views without a traditional intraoral sensor. If your panoramic unit generates a segmented posterior quadrant image with diagnostic detail equivalent to a periapical radiograph, D0251 becomes the appropriate selection.
New Code: D0431
D0431 – Salivary diagnostic test for caries risk assessment utilizing a point-of-care platform
This new code addresses the growing use of chairside salivary testing. A patient swishes a sterile solution, expectorates into a collection cup, and the sample runs through a small analyzer measuring bacterial load, buffering capacity, and pH. Results print within minutes.
Use D0431 when you order the test and interpret the results during the same visit. Documentation must include the quantitative outputs and your interpretation linking those values to the patient’s caries risk status.
Billing Tip: Many dental plans still consider caries risk assessment a non-covered service. Provide patients with a financial agreement before performing the test.
Preventive Procedures (D1000-D1999)
Prevention codes shift toward personalized risk-based intervals rather than blanket six-month defaults.
D1110: Prophylaxis – Adult
The code remains. The substantial change arrives in the form of a new sibling code. D1110 is retained for patients with healthy periodontium or stable gingivitis. The 2026 manual introduces a new code for patients with a history of treated periodontitis who now present with reduced but stable periodontium.
New Code: D1112
D1112 – Prophylaxis – Adult, history of treated periodontitis
This code applies to patients who completed active periodontal therapy and demonstrate no clinical signs of active disease (bleeding on probing at fewer than 10% of sites, probing depths at 4mm or less, no clinical attachment loss progression). The prophy procedure remains similar to D1110, but the patient’s higher-risk status demands more meticulous biofilm disruption.
Documentation Requirement: Record the date of last active periodontal therapy, current periodontal charting, and a statement confirming stability.
Why This Matters: Some payers previously bundled adult prophies and denied additional cleanings for periodontally involved patients. D1112 creates a distinct pathway that payers can adjudicate differently, potentially allowing more frequent maintenance without denials.
D1206 and D1208: Topical Fluoride Application
The fluoride codes now accommodate silver diamine fluoride (SDF) more cleanly. Previously, billing SDF for caries arrest under preventive codes generated confusion. The 2026 code set clarifies:
- D1206: Topical application of fluoride varnish (5% sodium fluoride).
- D1208: Topical application of fluoride – excluding varnish.
A separate code handles pharmacologic caries arrest.
New Code: D1356
D1356 – Pharmacologic caries arrest – silver diamine fluoride, per tooth
When applying SDF with the intent of arresting an active carious lesion, use D1356. This procedure differs from a preventive varnish application because the lesion already exists. Document the tooth number(s), lesion size and activity, and the planned reapplication interval. Most payers recognize SDF as a covered benefit when billed with this code.
Important Table: Preventive Code Selection for High-Risk Patients
| Clinical Scenario | Appropriate Code | Key Documentation |
|---|---|---|
| Healthy adult, routine cleaning | D1110 | No bone loss, no BOP |
| Adult with treated periodontitis, stable | D1112 | Historical perio charting, current stability statement |
| Child, fluoride varnish application | D1206 | Caries risk assessment |
| SDF for active cavitated lesion on tooth #30 | D1356 | Lesion description, photographic or radiographic evidence |
| SDF for prevention on high-risk, non-cavitated surface | D1208 (off-label documentation) | Caries risk status, rationale |
Restorative Procedures (D2000-D2999)
Restorative coding receives a substantial overhaul for digitally fabricated restorations.
D2740: Crown – Porcelain/Ceramic Substrate
This workhorse code remains. However, the 2026 manual explicitly separates the restorative process from the digital acquisition process. You may bill for a crown and a separate digital scan, but only under specific conditions described below.
New Code: D2715
D2715 – Crown – Porcelain/Ceramic, digitally designed and milled in-office
Use this code when you complete the entire restoration in a single visit using chairside CAD/CAM technology. This includes optical impression, digital design, milling, sintering/staining/glazing, and delivery all in one appointment. The code captures the professional services, materials, and technology use specific to same-day dentistry.
Contrast with D2740: D2740 is now reserved for restorations fabricated by a dental laboratory, whether from a conventional or digital impression.
New Code: D2957
D2957 – Digital scan for custom fabricated indirect restoration – transmitted to a laboratory
When you capture a digital impression and send the file to a lab for fabrication of a crown, inlay, onlay, or bridge, you may report D2957 in addition to the restorative code. This code values the acquisition cost, software processing, and transmission of the digital file. Do not use this code if the restoration is milled in-office (those costs are bundled into D2715).
Payer Alert: Some payers may initially bundle D2957 with D2740. Be prepared to submit a narrative explaining that the digital scan fee represents a separate distinct service from the laboratory fabrication itself. The ADA’s inclusion of this code supports unbundling, but payer adoption varies.
D2391 and D2392: Composite Restorations
The posterior composite codes now have mirror anterior codes that describe the size and complexity based on remaining tooth structure.
- D2391: Resin-based composite – one surface, posterior.
- D2392: Resin-based composite – two surfaces, posterior.
- D2393: Resin-based composite – three surfaces, posterior.
- D2394: Resin-based composite – four or more surfaces, posterior.
The addition of D2394 closes a gap for severely broken-down posterior teeth restored with direct composite, where the number of surfaces exceeded three but didn’t warrant a crown. The code helps capture the extended time and complexity.
Endodontic Procedures (D3000-D3999)
Endodontic coding remains relatively stable, with a critical addition for vital pulp therapy.
New Code: D3223
D3223 – Partial pulpotomy – permanent tooth (excluding final restoration)
Vital pulp therapy gained strong evidentiary support. The partial pulpotomy removes 2-4mm of coronal pulp tissue to the level of healthy pulp, places a biocompatible material (such as calcium silicate cement), and restores the tooth. This procedure bridges the gap between an indirect pulp cap (D3120) and a full pulpectomy (D3310).
Indications: Carious or traumatic pulp exposure in a permanent tooth with a normal pulp or reversible pulpitis diagnosis. The tooth must respond normally to cold testing and have no periapical pathology.
Documentation: Record the diagnosis, exposure size, depth of pulp tissue removed, hemostasis achieved, and the specific material placed.
D3333: Internal Root Repair of Perforation Defects
The descriptor now clarifies that D3333 applies to both iatrogenic perforations and pathologic internal resorption that has created a communication with the periodontal ligament. The 2026 manual adds a parenthetical note that this code is not limited to pulpal floor perforations.
Periodontal Procedures (D4000-D4999)
Periodontal codes grow to include biologic therapies and refined maintenance protocols.
D4381: Localized Delivery of Antimicrobial Agents
The code continues to apply to the placement of a biodegradable, controlled-release antimicrobial (like minocycline microspheres or doxycycline polymer) directly into a diseased periodontal pocket.
2026 Clarification: The ADA confirms D4381 is reported per tooth, not per site, even if multiple sites on the same tooth receive placement. If you treat mesial, distal, and buccal pockets on tooth #14, you bill one unit of D4381 for that tooth.
New Code: D4385
D4385 – Subgingival application of a biologic mediator, per tooth
This new code covers the placement of biologics intended to modulate the host response or promote regeneration at a molecular level. Examples include enamel matrix derivative placed into a suprabony defect during non-surgical therapy or platelet-rich fibrin placed into a non-contained defect.
Distinction from D4265 (Biologic Materials for Grafts): D4265 reports regenerative materials placed during surgical access (flap). D4385 is for non-surgical, closed placement when no flap is elevated.
Payer Caution: Biologics reimbursement lags significantly. Submit predeterminations and detailed narratives. Appeal denials by emphasizing the biologic’s role in reducing long-term surgical costs.
New Code: D4343
D4343 – Periodontal debridement for maintenance of peri-implant health
The rising prevalence of peri-implantitis demanded a code distinguishing natural tooth scaling from implant maintenance. D4343 fills this need. This procedure uses specialized non-metallic instruments (plastic, carbon fiber, or ultrasonic tips with polymer sleeves) to debride an implant surface without altering the abutment or prosthesis surface.
Documentation Distinctions:
- For natural teeth maintenance: D4910 (periodontal maintenance).
- For implants only, no flap: D4343.
- For implants with flap access for decontamination: See D6085 (implant maintenance procedure).
Comparative Table: Periodontal Maintenance Codes
| Code | Target | Flap Elevation? | Instrumentation | Typical Interval |
|---|---|---|---|---|
| D1110 | Healthy/non-periodontitis adults | No | Universal scalers, rubber cup | 6 months |
| D1112 | Treated periodontitis, stable | No | Universal scalers, selective curettes | 3-6 months |
| D4910 | Active maintenance after perio therapy | No | Site-specific scaling/root planing as needed | 3-4 months |
| D4343 | Dental implants, maintenance | No | Non-metallic scalers, ultrasonic with plastic tips | 3-6 months |
| D6085 | Implants, peri-implantitis treatment | Often yes | Titanium or carbon fiber curettes, implantoplasty | Therapeutic, as diagnosed |
Implant Services (D6000-D6199)
The implant code range expands significantly, recognizing the full lifecycle of implant therapy from planning to late complications.
D6010: Surgical Placement of Implant Body: Endosteal Implant
No change to the primary surgical placement code. However, the manual now adds a coding companion for surgical guides.
New Code: D6193
D6193 – Cone beam CT acquisition and interpretation with radiographic guide fabrication for implant treatment planning
This code bundles three distinct services performed in your office for a single implant site or an entire arch:
- CBCT scan acquisition.
- Interpretation with a structured report identifying critical anatomic structures (inferior alveolar nerve, maxillary sinus, adjacent roots).
- Design and fabrication of a radiographic guide (not a surgical guide) used during the scan.
When you refer the scan to an external radiologist for interpretation, do not report this code. Instead, bill D0367 (CBCT capture) and the radiologist bills separately for interpretation.
New Code: D6194
D6194 – Digital surgical guide design and fabrication – in-office
If you design and 3D-print or mill a surgical guide in your office using integrated planning software, report D6194 per arch. This code applies to tooth-supported, mucosal-supported, or bone-supported guides.
Contrast with Laboratory-Billed Guide: If an external lab designs and fabricates the guide, the lab bills you, and you may pass that lab fee to the patient on a separate line using the narrative “Laboratory-fabricated surgical guide.” There is no direct patient billing code for externally fabricated guides; you handle this as a laboratory expense.
D6080: Implant Maintenance Procedures
The implant maintenance suite expands dramatically.
New Code: D6081
D6081 – Removal of implant supported fixed prosthesis (screw-retained) for peri-implant evaluation and debridement
When you remove a multi-unit screw-retained bridge or a single screw-retained crown to assess peri-implant tissue health, probe, and debride, use D6081. This procedure goes beyond a supragingival maintenance. You access the implant abutment junction directly.
Documentation: Note the reason for removal (bleeding on probing, suppuration, radiographic bone loss), the condition of the implant interface, and any additional procedures performed (e.g., D6085). Bill D6081 per arch when the prosthesis spans multiple implants; bill per prosthesis when a single crown is removed.
New Code: D6085
D6085 – Full thickness flap, implant debridement, and detoxification – per implant
Peri-implantitis with suppuration and radiographic bone loss that cannot resolve with closed debridement necessitates surgical access. This code reports the surgical exposure of the implant surface, removal of granulation tissue, mechanical debridement, chemical detoxification (e.g., citric acid, tetracycline slurry, or chlorhexidine irrigation), and closure.
Do not confuse with D4343: D4343 is non-surgical. D6085 is a surgical procedure with flap reflection.
Important Note on Implant Removals
The 2026 manual clarifies removal code selection based on etiology:
- D6100: Implant removal – mechanical failure (fractured implant body, loose abutment connection due to component wear not peri-implantitis).
- New Code D6102: Implant removal – biological failure (peri-implantitis resulting in mobility or bone loss exceeding 50% of the implant length).
Using the correct removal code matters for secondary payer claims. Medical payers sometimes cover removal for biological complications under the patient’s medical plan, while mechanical failures may fall under different benefits.
Prosthodontics, Removable (D5000-D5899)
Removable prosthodontics sees updates focused on implant-supported overdentures and digital workflows.
D5863 and D5864: Overdenture – Complete Maxillary and Mandibular
These codes receive an editorial revision clarifying that they report the prosthesis only, not the attachments or any implant services. The 2026 manual directs clinicians to report attachment housings and processing separately (D5867).
New Code: D5868
D5868 – Replacement of processed attachment in existing overdenture – direct chairside method
When an existing overdenture’s nylon or polyetheretherketone (PEEK) insert wears out and you replace it chairside using a direct pick-up technique, use D5868. This code includes the cost of the new attachment insert and the clinical time.
Distinction from D5867: D5867 is laboratory-processed to place a new attachment housing into a new or existing denture base. D5868 is a chairside reline and replacement of a worn insert without removing the denture’s metal housing.
Oral and Maxillofacial Surgery (D7000-D7999)
Surgical coding includes new codes addressing pharmacologic adjuncts.
D7251: Coronectomy – Intentional Partial Tooth Removal
The ADA retains D7251 with an expanded descriptor clarifying its indication for teeth at high risk for nerve injury. The descriptor now explicitly states that radiographic documentation of the retained root fragment’s position relative to the inferior alveolar canal is required.
New Code: D7998
D7998 – Intraoperative pharmacologic agent application for nerve injury risk mitigation
Surgeons occasionally apply dexamethasone or other steroid solutions directly to an exposed nerve or within the socket following a high-risk third molar extraction. D7998 captures the pharmacologic preparation and application beyond the surgical procedure itself.
Usage Restriction: This code is additive to the primary extraction code (e.g., D7230). Do not use it for routine PRF placement or socket preservation grafting.
Adjunctive General Services (D9000-D9999)
This category houses practice management, sedation, and house-call codes.
D9310: Consultation
The 2026 manual emphasizes that a consultation must involve a dentist not previously treating the patient for the specific condition and the consulting dentist must provide a written report to the referring dentist. A second opinion requested by a patient without a referring doctor does not qualify as D9310; use the appropriate evaluation code.
New Code: D9423
D9423 – Office-based intravenous moderate (conscious) sedation – each 15-minute increment
Moderate sedation coding moves to time-based increments for better accuracy. D9423 replaces the former unit-per-visit approach for intravenous moderate sedation. Start time recording when the sedative agent administration begins. Stop when the patient meets discharge criteria and the sedation provider completes postoperative evaluation and instructions.
Documentation Mandate: Anesthesia record must include continuous monitoring of pulse oximetry, blood pressure, heart rate, and level of consciousness at five-minute intervals. The 2026 descriptor specifically requires recording the sedation start and stop times, medication doses, and the patient’s Aldrete score upon discharge.
New Code: D9998
D9998 – Teledentistry synchronous encounter – provider-to-provider consultation
When you hold a live video consultation with another healthcare provider about a mutual patient’s care, report D9998. This code is not for direct-to-patient teledentistry visits. Document the reason for consultation, participants, and resulting clinical decisions.
Navigating Payer Policies in 2026
Code existence doesn’t guarantee payment. Each payer independently decides coverage, frequency limitations, and documentation requirements.
The Predetermination Advantage
For any code designated as “New” in this article, submit a predetermination of benefits before starting treatment. Predetermination protects both your practice and your patient from unexpected costs. It also educates the payer’s reviewers about the new code’s intended use.
Allow 30 days for most commercial carriers and up to 45 days for government programs. The written response becomes a binding document for the specified timeframe, typically 90 days.
Writing an Effective Narrative
A new code without supporting narrative appears as an unrecognized line item. Craft narratives that answer five questions:
- What was the clinical diagnosis or condition?
- What previous treatment failed or proved insufficient?
- Why is this specific procedure necessary?
- How does this procedure differ from similar, existing codes?
- What outcome do you expect?
Example Narrative for D1112:
“Patient completed full-mouth scaling and root planing (D4341) on 01/15/2025. Current periodontal charting dated 04/10/2026 demonstrates probing depths of 2-3mm throughout with bleeding on probing at 8% of sites. No clinical attachment loss progression noted. Prophylaxis for adult with history of treated periodontitis (D1112) is indicated given the patient’s elevated risk profile despite current stability.”
Coordination with Medical Payers
Several 2026 codes hold particular interest for medical plans:
- D0431 (salivary diagnostics) may be covered under medical wellness benefits.
- D6102 (implant removal for biological failure) can be billed to medical under the patient’s surgical benefit.
- Sleep apnea appliance codes (E0486 for medical or the corresponding dental code) require proper medical documentation including a sleep study.
Always verify medical coverage before billing the dental carrier. Once a dental claim processes, billing the medical carrier for the same service often triggers coordination of benefit issues.
Documentation Excellence for 2026
Documentation determines claim outcomes. Specific documentation unlocks reimbursement. General notes lead to denials.
The Core Components
Every patient record entry should contain:
- Chief Concern: The patient’s stated reason for the visit, quoted when possible.
- Objective Findings: Radiographic interpretations, periodontal chartings, photographic evidence, pulp vitality test results, caries detection device readings, or other quantifiable data.
- Assessment: Your diagnosis or differential diagnosis.
- Procedure Details: Specific instrumentation, materials, anesthesia, and any complications.
- Plan: Next steps, follow-up intervals, and patient instructions.
Radiographic Documentation
For any procedure that involves a tooth or implant, radiographs must be diagnostic quality, dated, and stored in the patient’s record. The 2026 codes for implant removal (D6100, D6102) specifically require pre-operative radiographs demonstrating the reason for removal. For D6085, a pre-operative periapical or CBCT slice showing the bone loss pattern supports the surgical approach.
Periodontal Charting
Six-point pocket charting remains the gold standard. For D1112, D4910, and any implant maintenance code, updated charting within the past 12 months supports medical necessity. Payers increasingly request this during post-payment reviews.
The Financial Impact of Proper Coding
Miscoding erodes revenue in two directions. Undercoding leaves money on the table; overpayments trigger audits and recoupments.
Real Revenue Recovery Example
A practice treating 200 periodontally stable patients annually previously coded all as D1110. Switching to D1112 for those meeting criteria may open a higher fee schedule or allow more frequent maintenance visits. Assuming a $15 differential per visit and two visits per year, the practice recovers $6,000 annually from documentation improvement alone.
Audit Triggers to Avoid
- Billing D1112 without any history of periodontal therapy in the chart.
- Billing D6085 with no pre-operative radiographic evidence of peri-implant bone loss.
- Billing D9998 for a phone call that lacks a structured video component.
- Billing D1356 on multiple teeth without documenting specific lesion activity for each.
Staff Training Investment
Dedicate one team meeting in December to the code changes. Print a quick-reference card for each operatory listing the new codes with their clinical indicators. Role-play the financial conversation when a patient asks about a new salivary test or same-day crown fee. Prepared teams deliver confident, consistent messaging.
Technology Integration and Digital Codes
The 2026 update formalizes the digital workflow. This creates opportunities to capture value for technology investments.
Cone Beam Computed Tomography
D0367 (CBCT capture) remains the code for image acquisition. The interpretation codes (D0364-D0366) depend on the structures interpreted. The 2026 manual adds a note clarifying that when a CBCT is taken for implant planning, D6193 may be a more appropriate bundled code than reporting D0367 plus a separate interpretation.
Intraoral Scanning
With the new D2957 code, you can now bill for digital impression transmission separately from the restoration. Establish a practice policy. Some offices include the scan fee in their crown fee and do not bill D2957. Others itemize it. Consistency across providers avoids patient confusion and payer scrutiny.
3D Printing
The code set does not yet have a specific code for in-office 3D printing of models or surgical guides beyond D6194. If you 3D-print diagnostic models, temporaries, or occlusal guards, capture those costs within the appropriate treatment code’s fee or as a laboratory expense.
Special Populations and Code Considerations
Coding for pediatric, geriatric, and special needs patients involves unique challenges.
Pediatric Dentistry
The SDF code D1356 sees significant utilization in pediatric settings. The cooperative behavior or pre-cooperative nature of very young patients sometimes necessitates protective stabilization or sedation. The 2026 manual reminds clinicians that the evaluation and management of behavior, when sedation is used, is reported with the appropriate sedation code in addition to the restorative or surgical code.
Geriatric and Homebound Patients
The house call code D9410 (House call visit) now includes a note that additional procedures performed at the same visit are reported separately. Teledentistry follow-ups using D9995 (synchronous teledentistry visit) can bridge the gap between in-person visits for homebound patients.
Patients with Disabilities
Documentation of medical necessity becomes especially important when a patient requires extra time, special positioning, or multiple short appointments to complete a procedure. The ADA’s CDT manual includes a code for a detailed and extensive evaluation (D0150) and problem-focused evaluation (D0140). When a new patient with complex medical or behavioral needs requires a significantly extended appointment, your narrative in Box 35 of the claim form must reflect the reasons for the extended time.
Global Coding Considerations
The CDT code set is specific to the United States. However, international practitioners or those treating patients with international dental plans should note some nuances.
Canada
Canadian dental plans use the CDAnet codes maintained by the Canadian Dental Association. While structurally similar, the 2026 CDT and CDAnet codes are not identical. Cross-border patients require attention to which code set the payer recognizes.
ICD-10-CM Linkage
While not part of the CDT manual, payers increasingly encourage reporting ICD-10-CM diagnosis codes on claims. For 2026, pair your procedures with appropriate diagnoses:
- D1356 linked to K02.9 (dental caries, unspecified) or K02.52 (dental caries on pit and fissure surface penetrating into dentin).
- D6085 linked to K08.23 (peri-implantitis).
- D1112 linked to Z87.89 (personal history of other specified conditions) and Z91.84 (oral health risk factors).
This linkage provides the medical necessity justification automated claim adjudication systems seek.
Preparing Your Practice for January 1, 2026
Transitioning smoothly requires action across several fronts.
Software Updates
Verify with your practice management software vendor that the 2026 CDT database will load automatically. Some systems require a manual import. Test the update in a sandbox environment if possible. Ensure all fee schedules map correctly to the new codes.
Fee Schedule Development
Review each new code’s relative value compared to existing procedures. For D1112, your fee likely falls between D1110 and D4910. For D2715, benchmark against the D2740 fee plus the D2957 scan fee combined, then adjust for the efficiency and cost of in-house milling. Consult the ADA’s survey of dental fees, but also consider your own overhead costs, lab expense elimination, and local market.
Payer Communication
Contact the provider relations departments of your top five insurance carriers. Ask specific questions:
- “Will you reimburse D1112 on the same frequency as D1110 or D4910?”
- “Is D6193 covered under the medical or dental benefit for your plan?”
- “What documentation do you require for D6085 claims?”
Document the representative’s name, the date, and the response reference number. This protects you in future appeals.
Patient Communication
Update your financial agreement forms. Add language about new technologies:
“I understand that my treatment plan may include digital procedures such as optical impressions (D2957), salivary diagnostic tests (D0431), or same-day CAD/CAM restorations (D2715). These procedures involve technology fees that may not be covered by my dental plan. I accept financial responsibility for non-covered services.”
Transparency builds trust and accelerates collections.
The Future Beyond 2026
The CMC continually accepts code change requests. Several emerging areas may generate new codes in 2027 or 2028:
Artificial Intelligence in Diagnostics
AI-assisted radiographic interpretation continues to advance. A future code may differentiate between a dentist-only radiographic interpretation and one augmented by an AI platform that highlights potential carious lesions, bone loss patterns, or pathologies. The FDA’s evolving stance on AI as a medical device will shape this trajectory.
Regenerative Endodontics
Revascularization procedures in immature permanent teeth currently require piecemeal coding. A specific regenerative endodontic code appears likely within the next three years.
Minimally Invasive Surgical Techniques
Piezoelectric surgery and laser-assisted procedures may eventually gain dedicated codes that distinguish them from traditional rotary instrumentation.
Value-Based Care Codes
As dental plans experiment with value-based reimbursement, codes that capture outcomes (e.g., caries arrest confirmed at a one-year follow-up) rather than just procedures could emerge.
Stay engaged with your state dental association’s coding committee. Submit suggestions for codes that would improve your ability to accurately document and bill for the care you provide. The system changes through practitioner input.
Frequently Asked Questions
What is the most important 2026 code change for a general dentist?
The introduction of D1112 for adult prophylaxis on patients with a history of treated periodontitis is significant. It acknowledges the clinical difference between a patient who has never had periodontal disease and one who remains stable after treatment. This code can improve coverage for maintenance care.
Can I bill D2957 for a digital scan if my lab doesn’t accept digital files?
No. D2957 specifically states the scan is transmitted to a laboratory for fabrication. If you capture a digital impression but then pour a model from the scan and mail it to the lab, this is a conventional workflow and the digital capture is considered part of the restorative procedure, not a separately billable service.
How do I code an implant bridge removal for cleaning?
Use D6081 for the removal of the screw-retained implant prosthesis, per arch. Then report D4343 or D6085 for the debridement of the underlying implants depending on whether you reflect a flap.
Is the salivary diagnostic test covered by insurance?
Coverage is limited but growing. Some medical plans with robust wellness benefits cover salivary diagnostics. Dental plans are slower to adopt. Always check benefits before performing the test and have patients sign a financial agreement.
What code do I use for IV moderate sedation now?
D9423, reported in 15-minute increments. Start timing at the initiation of drug administration and stop when discharge criteria are met.
Conclusion
The 2026 CDT code update emphasizes precision, digital integration, and long-term patient maintenance. Clinicians gain dedicated codes for implant maintenance, same-day CAD/CAM restorations, salivary diagnostics, and pharmacologic caries arrest. Successful implementation requires thorough documentation, proactive payer communication, and staff training. A practice that masters these codes protects revenue, reduces claim denials, and accurately reflects the quality of care delivered to each patient.
Additional Resource
For the most current, official information, visit the American Dental Association’s CDT page:
ADA CDT Code Resources
ADA.org/en/publications/ada-catalog/cdt
This page provides access to the official manual, code change highlights, and submission guidelines for requesting future code changes. Always cross-reference any third-party guide against the official ADA publication.
Disclaimer: This article provides educational information about the 2026 CDT code set. It does not constitute legal, financial, or clinical coding advice. Code descriptions are paraphrased for readability and are not the official ADA descriptors. Always consult the official ADA CDT manual and your payer contracts before submitting claims. Reimbursement outcomes vary by payer, plan design, and geographic region.