ADA Code of Dental Procedures: A Patient’s Complete Guide to Understanding CDT Codes
Sitting in a dental chair often comes with a mix of emotions. You might feel relief that a nagging toothache will finally get treated. You might feel anxiety about the procedure itself. But for many people, the most confusing moment happens after the dentist steps away. A staff member hands you a treatment plan filled with strange combinations of letters and numbers. You see terms like “D2740” or “D4341” and a list of fees that may or may not be covered by your insurance.
This experience can feel isolating. The codes look like a secret language designed for computers and insurance companies, not for you. But here is the truth: this language belongs to you as much as it belongs to any insurance clerk. Understanding it changes everything about how you approach your oral health. It empowers you to ask better questions, budget more accurately, and avoid surprise bills that throw your finances into chaos.
This guide will walk you through the entire universe of the ADA Code of Dental Procedures. We will explore its history, its structure, and its practical application in your daily life. You will learn how to read a treatment plan. You will discover the difference between a routine cleaning and a deep cleaning. You will understand why one crown costs more than another. By the time you finish reading, you will no longer see those codes as obstacles. You will see them as tools that help you take control of your dental care journey.
What Is the ADA Code of Dental Procedures?
The American Dental Association maintains a standardized coding system officially named the Code on Dental Procedures and Nomenclature. Most dental professionals simply call it the CDT Code. This system gives a unique five-character alphanumeric code to every specific dental procedure. When a dentist recommends a treatment, the corresponding code translates that medical service into a format that insurance companies can process quickly and consistently.
Think of the CDT Code as a universal translator for dentistry. Before its widespread adoption, dentists used their own descriptions for procedures. One office might call a filling a “silver restoration” while another called it an “amalgam repair.” Insurance companies struggled to compare claims. Patients had no way to understand what they paid for. The ADA introduced the code to solve this chaos. Now, a “D2140” means the same thing in Florida as it does in Oregon.
The code does more than just standardize language. It creates accountability. Every code has a clear, official definition that describes the procedure in detail. If you see D2751 on your bill, the CDT manual specifies exactly what that code represents: a crown made of porcelain fused to a predominantly base metal. This precision protects you from vague billing practices. You can look up any code and verify that the treatment you received matches the description.
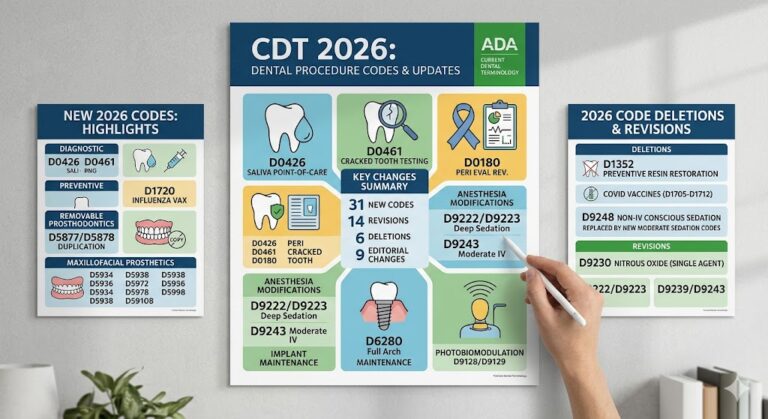
The ADA updates the CDT Code annually. New technologies emerge. Old techniques become obsolete. The Code Maintenance Committee, which includes representatives from dental associations, insurance companies, and other stakeholders, reviews proposals for additions, deletions, and revisions every year. This ongoing maintenance ensures the code remains relevant and accurate. For you, this means the system stays current with modern dentistry. A procedure that did not exist five years ago likely has a dedicated code today.
Important Note: Dental codes differ from medical codes. Medical billing uses Current Procedural Terminology (CPT) codes. Dental billing uses CDT codes. These systems do not overlap. If you ever need a dental procedure that crosses into medical territory, such as treatment for a jaw fracture or sleep apnea, your provider might need to submit a medical claim instead. However, for 99% of what happens in a dental office, the CDT code governs the documentation.
Why These Codes Matter Directly to You
Imagine booking a flight without knowing the price until you land at your destination. The airline tells you, “Trust us, it will be reasonable.” You would never accept that. Yet many dental patients accept exactly that scenario. They schedule treatment without fully understanding the codes on their treatment plan. Then the bill arrives, and the insurance company covers less than expected. The patient feels blindsided and powerless.
Understanding the ADA Code of Dental Procedures prevents this nightmare. When you know the codes, you can call your insurance company before treatment and ask specific, targeted questions. Instead of saying, “Do you cover a crown?” you can ask, “What is your coverage percentage for procedure D2740 on tooth number 19?” The customer service representative can give you a clear, immediate answer. You remove the guesswork from your financial planning.
Codes also help you understand why your dentist recommends one procedure over another. Two treatments might sound similar in plain English, but their codes reveal crucial differences. A “periodic oral evaluation” (D0120) differs from a “comprehensive oral evaluation” (D0150). The periodic exam is for established patients returning for a routine checkup. The comprehensive exam is for new patients or patients with significant changes in their health. The scope of the exam differs, and so does the cost. Understanding this distinction helps you see the value in what your dentist provides.
For patients without insurance, codes offer a different kind of power: the ability to comparison shop. Dentistry is a competitive marketplace. Fees vary widely between practices, even within the same zip code. When you have a treatment plan with specific codes, you can call other reputable offices and ask for their fees for the exact same procedures. This transparency keeps the market honest and helps you find care that fits your budget without sacrificing quality.
The codes also create a permanent record of your oral health history. Years from now, a new dentist can look at your chart and see that you had a D3310 (root canal on an anterior tooth) in 2023. They instantly know the exact treatment you received. This continuity of care improves your long-term health outcomes.
The Architecture of a CDT Code Entry
Every code in the CDT manual follows a consistent format. Understanding this format helps you navigate the system with confidence. A full CDT code entry contains three essential components. The first component is the procedure code itself, which always begins with the letter “D” followed by four numbers. The second component is the nomenclature, which is the official written title of the procedure. The third component is the descriptor, which provides a detailed definition of what the procedure includes and, crucially, what it does not include.
Consider code D1110 as an example. The code itself is “D1110.” The nomenclature is “prophylaxis – adult.” The descriptor explains that this procedure involves the removal of plaque, calculus, and stains from the tooth structures in the permanent and transitional dentition. It also specifies that the procedure includes scaling and polishing of all surfaces above the gumline. This level of detail eliminates ambiguity. A dentist cannot bill D1110 for a child under a certain age, because a separate code (D1120) exists for pediatric prophylaxis.
The “D” prefix universally identifies a dental procedure code. This prefix immediately distinguishes a dental claim from a medical claim. When you review an explanation of benefits from your insurance company, you can quickly scan the document for “D” codes to identify the dental services you received.
The four digits following the “D” are not random. They follow a logical category system. The first digit after the “D” indicates the major category of service. Codes beginning with D0 relate to diagnostic procedures. Codes beginning with D1 relate to preventive procedures. Codes beginning with D2 relate to restorative procedures. This structure allows anyone to quickly identify the general type of service associated with any code. If you see a code starting with D7, you know immediately that it falls into the category of oral and maxillofacial surgery.
Note on Code Length: CDT codes always consist of exactly one letter and four numbers. If you ever see a code on a dental bill with a different format, question it. Legitimate dental procedures, as recognized by the ADA, always follow the DXXXX structure. A code with three numbers or five numbers raises a red flag that deserves your attention.
A Deep Dive into the Code Categories
The CDT Code organizes hundreds of procedures into twelve logical categories. Each category represents a distinct area of dental practice. Understanding these categories gives you a mental map of how dentistry is structured from a billing perspective. When you look at a treatment plan, you can immediately contextualize the services being recommended.
Diagnostic Services (D0100-D0999)
This category covers all the ways dentists gather information about your oral health. It includes examinations, radiographs (X-rays), tests, and assessments. The diagnostic category forms the foundation of every treatment plan. Before a dentist can recommend any restorative or surgical procedure, they must first perform a diagnostic evaluation to determine what conditions exist.
A comprehensive oral evaluation for a new patient (D0150) goes far beyond a quick look at your teeth. The descriptor for this code specifies that it includes a thorough assessment of your hard and soft tissues, an evaluation for oral cancer, a review of your medical history, and the development of a preliminary treatment plan. This examination establishes a baseline for your oral health. Your dentist uses the information gathered during this evaluation to identify existing problems and anticipate future concerns.
Periodic evaluations (D0120) serve a different purpose. These exams occur at recall appointments for established patients. The dentist checks for changes since your last visit, examines any areas of concern, and updates your treatment plan as necessary. The scope of a periodic evaluation is narrower than a comprehensive evaluation, which is reflected in a lower fee.
Radiographs form another significant subcategory within diagnostic services. A full mouth series of X-rays (D0210) captures detailed images of every tooth and supporting structure. Bitewing radiographs (D0270, D0272, D0274) show the crowns of the upper and lower teeth on a single film, allowing the dentist to detect decay between teeth. Periapical radiographs (D0220, D0230) capture the entire tooth from crown to root tip. Each type of X-ray serves a specific diagnostic purpose and carries its own code.
Important Distinction: A “limited oral evaluation” (D0140) is problem-focused. You might receive this code if you visit the dentist with a specific complaint, such as a toothache in a single area. The dentist examines only the area of concern. This differs from a comprehensive or periodic evaluation, which examines your entire mouth.
Preventive Services (D1000-D1999)
Preventive dentistry stops problems before they start. This category includes cleanings, fluoride treatments, sealants, and space maintainers. Insurance companies often cover preventive services at a high percentage because they understand that prevention reduces the need for expensive restorative work later.
Dental prophylaxis for an adult (D1110) is the classic “cleaning” that most people think of when they visit the dentist. The procedure removes plaque, tartar, and stains from the visible surfaces of teeth above the gumline. It also includes polishing to smooth tooth surfaces and make them more resistant to future plaque accumulation. This code applies to patients with healthy gums and no signs of periodontal disease.
Prophylaxis for a child (D1120) covers the same type of cleaning for patients in the primary or transitional dentition stage. The age cutoff varies by payer, but generally applies to children up to age 12 or 14. The technique and instruments used for children differ from those used for adults, which justifies the separate code.
Fluoride treatments strengthen tooth enamel and make it more resistant to acid attacks from bacteria. Topical application of fluoride (D1206 for fluoride varnish, D1208 for other topical applications) delivers a concentrated dose of this mineral directly to the teeth. The procedure takes only minutes but provides significant protection against decay, particularly for patients at high risk.
Dental sealants (D1351) offer another powerful preventive tool. A sealant is a thin plastic coating applied to the pits and grooves of back teeth. These areas trap food and bacteria easily, making them common sites for cavities. The sealant flows into these crevices and creates a smooth, protective barrier. This procedure is most common on permanent molars shortly after they erupt.
Key Understanding: Preventive codes represent services performed on patients without active disease. If you have gum disease, your cleaning is not preventive. It falls under a different category entirely. This distinction causes more insurance confusion than almost any other coding nuance.
Restorative Services (D2000-D2999)
Restorative dentistry repairs damaged or decayed teeth. This massive category includes fillings, crowns, inlays, onlays, and core buildups. The restorative codes are among the most frequently used in dentistry, and they contain important distinctions that affect both treatment outcomes and costs.
Amalgam restorations (D2140-D2161) use a silver-colored material to fill cavities. These fillings are durable, long-lasting, and cost-effective. The specific code depends on the number of tooth surfaces involved. A one-surface amalgam on a posterior tooth is D2140. A two-surface amalgam is D2150. A three-surface amalgam is D2160. Each additional surface requires more time and material, which justifies the higher fee.
Composite restorations (D2330-D2394) use tooth-colored resin material. These fillings bond directly to the tooth structure and provide an aesthetic alternative to amalgam. The codes follow the same surface-counting logic as amalgam codes. A one-surface composite on an anterior tooth is D2330. A four-or-more-surface composite on a posterior tooth is D2394. Composite fillings generally cost more than amalgam fillings due to the material cost and the more technique-sensitive placement process.
Crowns represent the most extensive type of indirect restoration. A crown covers the entire visible portion of a tooth, restoring its shape, strength, and appearance. The CDT code distinguishes between different crown materials. A crown made entirely of cast high noble metal is D2790. A crown made of porcelain fused to high noble metal is D2750. A crown made entirely of ceramic or porcelain is D2740. The material choice affects aesthetics, durability, and cost.
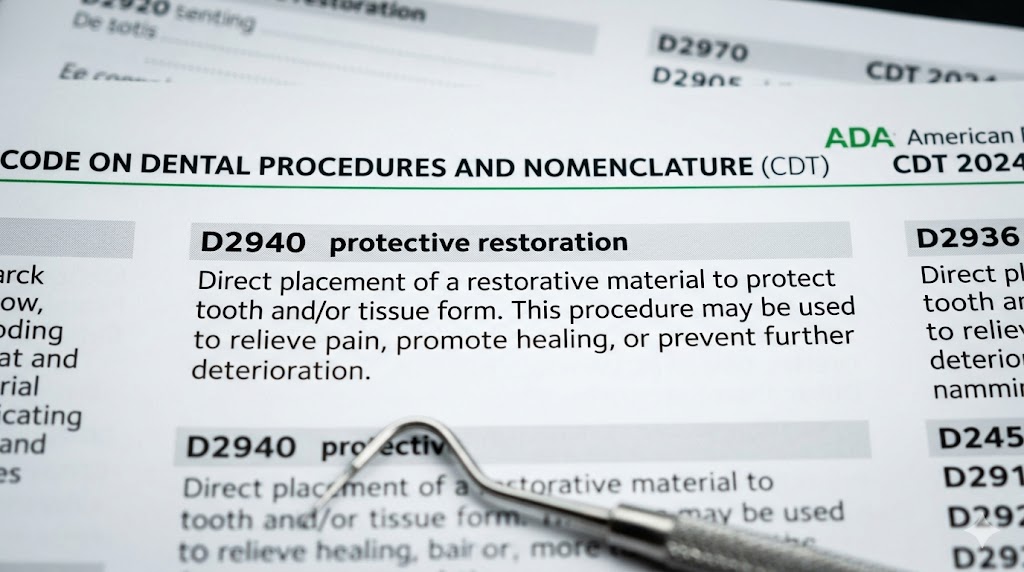
Important Clarification: When you receive a crown, you typically need a temporary crown while the permanent one is fabricated in a dental laboratory. The temporary crown has its own code (D2970) and may appear as a separate line item on your treatment plan. Some dental offices include the temporary crown in the fee for the permanent crown, while others bill it separately. Ask your provider how they handle this to avoid surprises.
| Restoration Type | Example Code | Material | Typical Lifespan | Relative Cost |
|---|---|---|---|---|
| Amalgam Filling | D2140 (1-surface) | Silver alloy | 10-15 years | Low |
| Composite Filling | D2330 (1-surface) | Tooth-colored resin | 7-10 years | Medium |
| Porcelain Crown | D2740 | All-ceramic | 10-15 years | High |
| PFM Crown | D2750 | Porcelain fused to metal | 10-15 years | High |
| Gold Crown | D2790 | High noble metal | 20+ years | Highest |
Endodontic Services (D3000-D3999)
Endodontics deals with the interior of the tooth, specifically the pulp chamber and root canals. When decay or trauma reaches the pulp, the tissue becomes inflamed or infected. Endodontic treatment removes the diseased pulp, cleans and shapes the root canal space, and seals the tooth to prevent reinfection. Most people know this procedure simply as a “root canal.”
The primary distinction in endodontic coding relates to the type of tooth being treated. Anterior teeth (incisors and canines) typically have a single root canal. Premolars (bicuspids) usually have one or two canals. Molars have multiple canals, often three or four. The complexity of the procedure increases with the number of canals, and the coding reflects this reality.
Root canal on an anterior tooth (D3310) addresses the simplest endodontic case. The tooth has one canal that is relatively straight and accessible. Root canal on a premolar (D3320) involves a tooth that may have one or two canals with more complex anatomy. Root canal on a molar (D3330) represents the most challenging and time-consuming endodontic procedure. The canals in molars are often curved, narrow, and difficult to navigate.
Retreatment Considerations: Sometimes a tooth that previously had a root canal becomes reinfected. This can happen if the original treatment missed a canal, if the seal breaks down over time, or if new decay exposes the root canal filling to bacteria. Retreatment of a previous root canal (D3346-D3348) involves removing the old filling material, cleaning the canals again, and placing a new seal. This procedure is more complex than the original root canal and carries a higher fee.
The descriptor for endodontic codes specifies that the fee includes the complete root canal procedure and any necessary radiographs taken during the appointment. It does not include the final restoration. After a root canal, the tooth usually needs a crown to protect it from fracture. The crown is billed separately under restorative codes.
Periodontal Services (D4000-D4999)
Periodontics focuses on the structures that support the teeth: the gums, periodontal ligament, and alveolar bone. When bacteria accumulate below the gumline, they trigger an inflammatory response that destroys these supporting tissues. Periodontal treatment aims to halt this destruction and, when possible, regenerate lost structures.
Scaling and root planing (D4341 for four or more teeth per quadrant, D4342 for one to three teeth per quadrant) is the foundational non-surgical periodontal procedure. People often call this a “deep cleaning.” The procedure involves removing plaque and calculus from root surfaces below the gumline. The dentist or hygienist uses instruments to smooth the root surfaces, making it harder for bacteria to reattach. This procedure typically requires local anesthesia because the instruments reach sensitive areas well below the gumline.
Critical Insurance Distinction: A regular prophylaxis (D1110) is a preventive procedure for patients with healthy gums. Scaling and root planing (D4341) is a therapeutic procedure for patients with active periodontal disease. If you have gum disease characterized by bone loss, bleeding on probing, and deep pocket depths, your insurance may not cover a D1110. You need D4341 instead. Submitting a preventive code for a therapeutic procedure constitutes incorrect coding and may result in claim denial.
Periodontal maintenance (D4910) follows active periodontal treatment. Once you have been treated for gum disease, you remain at risk for recurrence. Periodontal maintenance visits occur more frequently than routine cleanings, typically every three to four months. During these visits, the provider cleans above and below the gumline, monitors pocket depths, and checks for signs of disease reactivation. This code is specifically for patients who have completed active periodontal therapy.
Surgical periodontal procedures address more advanced disease. Osseous surgery (D4260-D4261) involves reflecting the gum tissue, cleaning the root surfaces and bone defects, and reshaping the bone to eliminate pockets. Soft tissue grafts (D4270-D4277) cover exposed root surfaces or augment thin gum tissue. These procedures are more invasive and costly than non-surgical treatment but are sometimes necessary to save teeth with severe bone loss.
Prosthodontic Services (D5000-D5899 and D6200-D6999)
Prosthodontics replaces missing teeth. This category splits into two subcategories: removable prostheses (dentures) and fixed prostheses (bridges and implants). The codes span a broad range because the category addresses every possible scenario of partial or complete tooth loss.
Complete dentures (D5110 for a maxillary denture, D5120 for a mandibular denture) replace all teeth in one arch. The process involves multiple appointments for impressions, bite registration, try-in, and delivery. The code covers the entire process from start to finish. Immediate dentures (D5130, D5140) are placed on the same day as tooth extractions, allowing the patient to avoid going without teeth during the healing period. A reline procedure is typically needed after the tissues heal and shrink.
Partial dentures (D5211-D5226) replace some missing teeth when natural teeth remain. A cast metal framework partial denture (D5213 for maxillary, D5214 for mandibular) uses a metal base for strength and retention. A flexible base partial denture (D5225, D5226) uses a nylon-type material that blends with the gum tissue and provides a more aesthetic alternative. The choice depends on the number and location of missing teeth, the condition of remaining teeth, and patient preference.
Fixed partial dentures, commonly called bridges, replace missing teeth by crowning the teeth on either side of the gap and suspending a false tooth between them. A bridge spanning one missing tooth with retainers on two abutment teeth is coded differently depending on the material. A porcelain fused to metal bridge (D6750 for the retainer crown, D6240 for the pontic) remains a common choice for posterior areas where strength matters most.
Implant Coding Note: Implant services appear in multiple categories. The implant body itself falls under endosseous implant codes (D6010). The abutment that connects the implant to the crown has its own code (D6056). The crown that attaches to the implant is coded as an implant-supported crown (D6058 for a cemented crown, D6059 for a screw-retained crown). This fragmentation means an implant treatment plan will show multiple line items, each representing a distinct component of the overall restoration.
Additional Service Categories
The CDT Code contains several other important categories. Oral and maxillofacial surgery codes (D7000-D7999) cover extractions, biopsies, and other surgical procedures. A simple extraction of an erupted tooth is D7140. A surgical extraction requiring flap reflection and bone removal is D7210. The distinction between simple and surgical extraction depends on the complexity of the procedure, not just the type of tooth.
Orthodontic codes (D8000-D8999) cover braces, aligners, and other tooth-moving appliances. Comprehensive orthodontic treatment of the adolescent dentition (D8080) represents the classic full braces case. Limited orthodontic treatment (D8010) addresses minor tooth movements. Clear aligner therapy has introduced new codes that describe this specific treatment modality.
Adjunctive general services (D9000-D9999) include procedures that do not fit neatly into other categories. This section covers anesthesia, professional visits, house calls, and occlusal guards. An occlusal guard (D9940) is a removable appliance worn to prevent teeth grinding and clenching. The code specifies that it is fabricated to reduce the effects of bruxism, which distinguishes it from a sports mouthguard (D9941).
How to Read Your Dental Treatment Plan
A treatment plan is a roadmap for your dental care. It lists the procedures your dentist recommends, the teeth involved, the associated fees, and your estimated insurance coverage. Reading this document effectively gives you control over your dental decisions. Let’s walk through the process step by step.
When you receive a treatment plan, look for the column labeled “Code” or “CDT Code.” This column contains the five-character codes we have been discussing. If your treatment plan does not include these codes, ask for them. A plan without procedure codes is incomplete. You cannot verify insurance coverage or compare fees without the codes.
Next, scan the “Tooth” or “Tooth Number” column. Dentists identify teeth by number. In the Universal Numbering System used in the United States, teeth are numbered 1 through 32. Tooth 1 is the upper right third molar (wisdom tooth). The numbering proceeds across the upper arch to tooth 16, the upper left third molar. Then it drops to the lower left third molar, tooth 17, and proceeds around the lower arch to tooth 32, the lower right third molar. Primary (baby) teeth use letters A through T.
Understanding tooth numbers helps you confirm that the treatment plan addresses the correct teeth. If you felt pain in a lower right tooth and your plan lists treatment on tooth 30, the plan is targeting the correct area. If the plan lists tooth 14, something is wrong. Verify this before authorizing treatment.
The “Description” column should contain the official CDT nomenclature or a simplified version of it. Compare this description to what your dentist explained during the examination. If the dentist recommended a crown made of white ceramic material, the code should be D2740, not D2790. Discrepancies between the verbal explanation and the coded plan deserve a conversation with your provider.
The “Fee” column shows the practice’s usual and customary charge for each procedure. This represents the amount you would pay if you had no insurance. The “Estimated Insurance” column shows what the provider expects your insurance company to pay. The “Patient Portion” column shows what you will owe after insurance processes the claim. Remember that these are estimates. The actual insurance payment may differ based on your plan’s specifics, remaining annual maximum, and other factors.
| Plan Element | What to Look For | Questions to Ask |
|---|---|---|
| Code | Verify it matches the recommended treatment | “Is this the exact code you will submit to my insurance?” |
| Tooth Number | Confirm it matches the tooth causing problems | “Can you show me on the X-ray which tooth this is?” |
| Description | Read the official definition of the code | “Does this code include the temporary and the permanent?” |
| Fee | Compare to other providers if you wish | “Does this fee include lab costs and follow-up visits?” |
| Insurance Estimate | Understand that it is not a guarantee | “What happens if my insurance pays less than estimated?” |
Critical Advice: Never authorize treatment based on verbal assurances alone. Get the treatment plan in writing with all codes clearly listed. Take the plan home if you need time to review it. Call your insurance company with the codes and tooth numbers to verify coverage directly. Do not rely solely on the dental office’s estimate. The dental office does not work for the insurance company, and the insurance company does not work for the dental office. You sit in the middle, and verification is your responsibility.
The Relationship Between CDT Codes and Insurance Coverage
Dental insurance does not function like medical insurance. Medical insurance protects you from catastrophic costs that could bankrupt you. Dental insurance operates more like a coupon with an annual limit. Most plans cap their payout at $1,000 to $2,000 per year. Once the insurance company pays that amount, you cover everything else out of pocket. Understanding how codes interact with your plan structure helps you maximize your benefits.
Every dental insurance plan includes a fee schedule that lists the maximum allowed amount for each code. If your dentist charges more than this allowed amount, you pay the difference. This concept, called balance billing, is common in dentistry. A dentist who is “in-network” has agreed to accept the insurance company’s fee schedule as payment in full for covered services. An “out-of-network” dentist has not made this agreement and may charge more than the allowed amount, leaving you responsible for the balance.
Insurance plans categorize codes into service classes. Class I typically includes diagnostic and preventive services. These services often receive 100% coverage with no deductible required. Class II includes basic restorative services like fillings and simple extractions. These services might be covered at 80% after you meet your deductible. Class III includes major services like crowns, bridges, and dentures. These services might be covered at 50% after your deductible. The specific percentages and classifications vary by plan.
Some codes trigger additional plan limitations. Many plans include a “missing tooth clause.” This provision excludes coverage for replacing a tooth that was missing before your coverage began. If you lost tooth 19 before you enrolled in your current plan, the insurance company may deny coverage for a bridge or implant to replace it. This clause catches many patients off guard. Understand your plan’s specific limitations before scheduling major restorative work.
Frequency limitations represent another common restriction. Your plan might cover a prophylaxis (D1110) only twice per year. It might cover a full mouth series of X-rays (D0210) once every five years. It might cover fluoride treatment (D1206) for adults only once per year, or not at all. Exceeding these frequency limits results in denial, even if your dentist deems the treatment medically necessary.
The Pre-Authorization Strategy: For any treatment plan exceeding a few hundred dollars, request that your dental office submit a pre-authorization to your insurance company. The insurance company reviews the proposed treatment, confirms your eligibility, and issues a written estimate of what they will pay. This process takes a few weeks but eliminates most billing surprises. Do not skip this step for crowns, bridges, implants, or periodontal surgery.
Navigating Common Coding Controversies and Challenges
The CDT Code aims for clarity, but gray areas exist. Some procedures generate frequent disagreements between dental offices, patients, and insurance companies. Understanding these controversies helps you advocate for yourself effectively.
The Prophylaxis vs. Scaling and Root Planing Debate
This represents perhaps the most common coding dispute in dentistry. A patient visits the dentist expecting a “regular cleaning” covered at 100% by insurance. The dentist diagnoses periodontal disease and recommends scaling and root planing (D4341), which costs significantly more and is covered at a lower percentage. The patient feels the dentist is upselling unnecessary treatment. The dentist sees a patient who genuinely needs therapeutic intervention to prevent tooth loss.
The clinical distinction rests on measurable criteria. Periodontal disease is diagnosed by measuring pocket depths around teeth, assessing bleeding on probing, and evaluating bone levels on X-rays. Healthy gums have pocket depths of 1-3 millimeters with no bleeding. Diseased gums have deeper pockets, bleeding, and visible bone loss. These measurements are objective and documented in your chart. If your dentist diagnoses periodontal disease, ask to see the periodontal charting. The numbers should justify the D4341 code.
That said, some dental offices do over-diagnose periodontal disease. Chain dental practices with aggressive production goals have faced scrutiny for recommending deep cleanings to patients who do not need them. If you receive a diagnosis you question, seek a second opinion. Take your X-rays and periodontal charting to another office. The cost of a second opinion exam is minor compared to unnecessary treatment.
Downgrading and Alternative Benefits
Insurance companies sometimes apply “alternative benefit” clauses. This means they will pay for the least expensive treatment that addresses the condition, even if your dentist recommends a more expensive option. The classic example involves posterior composite fillings. Your dentist recommends a tooth-colored composite filling (D2391) for a molar. Your insurance company notes that an amalgam filling (D2150) would also restore the tooth. They process the claim as if you received the amalgam, paying the amalgam rate, and leaving you with a larger patient portion.
This practice, called “downgrading,” is legal and disclosed in your plan documents, though few patients read those documents thoroughly. You have options. You can accept the amalgam filling and pay less out of pocket. You can pay the difference for the composite filling. You cannot force the insurance company to pay at the higher composite rate if your plan includes an alternative benefit clause for posterior restorations.
Bundling and Unbundling
Some procedures naturally go together. When a dentist prepares a tooth for a crown, they build up any missing tooth structure with a core buildup (D2950) before cementing the crown. Some insurance plans consider the buildup an integral part of the crown procedure and “bundle” the two codes, paying only for the crown. Other plans allow separate payment for the buildup when documentation supports it.
Unbundling occurs when a provider bills separate codes for components that the CDT descriptor specifies as included in a single code. For example, the descriptor for a root canal (D3310) states that the fee includes all necessary radiographs during the procedure. Billing a periapical X-ray (D0220) separately on the same day as the root canal would constitute unbundling. This practice, when intentional, constitutes fraud. If you notice this on your bill, question it.
| Controversy | What Happens | What You Can Do |
|---|---|---|
| Prophylaxis vs. SRP | Dentist codes D4341, insurance expects D1110 | Ask to see periodontal charting; get a second opinion |
| Downgrading | Insurance pays amalgam rate for composite | Accept amalgam, pay difference, or appeal with documentation |
| Bundling | Insurance denies separate payment for buildup | Ask dentist to submit narrative explaining medical necessity |
| Frequency Limits | Insurance denies cleaning because 6 months haven’t passed | Verify plan limits; consider paying out of pocket or waiting |
| Missing Tooth Clause | Insurance denies bridge covering missing tooth | Check if tooth was missing before coverage effective date |
The Annual CDT Code Update Process
The ADA releases a new version of the CDT Code every year, effective January 1. This annual update keeps the code aligned with advances in dental technology and practice. New procedures that gain widespread adoption eventually receive their own codes. Procedures that become obsolete are deleted. Descriptors are revised to clarify ambiguity.
The Code Maintenance Committee (CMC) oversees this process. The committee includes representatives from the ADA, dental specialty organizations, insurance carriers, and other stakeholders. Anyone can submit a code change request. The CMC reviews submissions, holds public hearings, and votes on each proposal. Accepted changes appear in the following year’s manual.
For patients, the annual update has practical implications. A procedure your plan covered last year might have a new code this year. A procedure that was not covered before might now have a dedicated code that triggers benefits. Dental offices must update their software and fee schedules annually to reflect the changes. This transition sometimes creates temporary confusion as systems catch up.
What This Means For You: When you receive treatment in January or February, confirm that your provider is using the current year’s codes. A code that was valid in December may have been deleted or revised in January. Most offices manage this transition smoothly, but awareness helps you catch any errors that might affect your claim.
Practical Strategies for Talking to Your Dental Office About Codes
Many patients feel intimidated when discussing money and codes with dental professionals. They worry about appearing difficult or untrusting. Let go of this concern. Ethical dental offices welcome informed patients who engage with their treatment plans. The conversation should feel collaborative, not adversarial.
Start the conversation positively. Frame your questions as a desire to understand, not as a challenge to the provider’s expertise. Say something like, “I want to make sure I understand my treatment plan so I can budget appropriately. Could you walk me through the codes and what each one means?” This approach invites education rather than triggering defensiveness.
Ask specifically about codes that seem redundant. If your plan lists both a core buildup (D2950) and a crown (D2740), ask, “Does the crown code already include the buildup, or are these truly separate services?” The answer might reveal that the tooth has extensive missing structure requiring a significant buildup beyond what a standard crown preparation includes. Or it might prompt the office to reconsider whether the buildup is separately billable.
Inquire about alternatives. Say, “Are there other ways to treat this condition that might use different codes?” A molar with extensive decay might be restorable with a large filling (D2161) rather than a crown (D2740), though the filling may not last as long. Understanding the spectrum of options, each with its associated code and cost, allows you to make an informed choice aligned with your values and budget.
When the treatment plan involves multiple appointments, ask for a phased approach. Prioritize urgent needs first. Schedule cosmetic procedures later when finances allow. A phased treatment plan might list Phase I codes for infection and pain control, Phase II codes for restoring function, and Phase III codes for aesthetic improvements. This approach reduces financial overwhelm while ensuring you receive necessary care.
Document Every Conversation: After discussing your treatment plan, send a follow-up email summarizing your understanding. Write something like, “Thank you for explaining that D2740 on tooth 19 includes the temporary crown and all adjustments for the first six months. I understand my estimated patient portion is $450 after insurance. Please let me know if I missed anything.” This written record protects you if a billing dispute arises later.
Understanding Your Explanation of Benefits (EOB)
After your dental office submits a claim, your insurance company sends you an Explanation of Benefits. This document is not a bill. It explains how the insurance company processed the claim. Understanding an EOB helps you verify that your provider submitted the correct codes and that your plan paid as expected.
The EOB lists each procedure code that the dental office submitted. Next to each code, you see the dentist’s charged amount. The insurance company then shows the allowed amount, which is the maximum they will consider for that code based on your plan’s fee schedule. If your dentist is in-network, the allowed amount is the contracted rate. If out-of-network, the allowed amount may be lower than the charged amount, leaving you responsible for the difference.
The EOB then applies your plan’s coverage percentage. For a preventive code like D1110, you might see coverage at 100% of the allowed amount. For a major code like D2750, you might see coverage at 50%. The insurance company calculates their payment and shows it in a column labeled “Plan Paid” or something similar. The remaining balance appears as “Patient Responsibility.”
Compare the EOB to your treatment plan and your actual bill from the dental office. The codes should match. The patient responsibility on the EOB should align with what the dental office bills you. If the EOB shows a higher patient responsibility than expected, investigate before paying. The dental office might have submitted a different code than what appeared on your treatment plan. Or the insurance company might have downgraded a service or applied a limitation you did not anticipate.
Common EOB Terms:
- Deductible: The amount you must pay before insurance begins covering services.
- Annual Maximum: The total amount the plan will pay in a calendar year.
- Coinsurance: The percentage you pay after the deductible is met.
- Non-Covered Service: A procedure your plan does not cover under any circumstances.
- Frequency Limitation: A denial because you exceeded the allowed number of services in a given period.
CDT Codes for the Most Common Dental Procedures: A Reference Table
The following table lists codes you are most likely to encounter during routine dental visits. Familiarize yourself with these codes. They will appear on your treatment plans and EOBs repeatedly throughout your life.
| Code | Nomenclature | Category | Typical Coverage Class |
|---|---|---|---|
| D0120 | Periodic Oral Evaluation | Diagnostic | Class I (100%) |
| D0150 | Comprehensive Oral Evaluation | Diagnostic | Class I (100%) |
| D0210 | Full Mouth Series of Radiographs | Diagnostic | Class I (100%) |
| D0220 | Periapical Radiograph (single) | Diagnostic | Class I (100%) |
| D0272 | Bitewing Radiographs (two) | Diagnostic | Class I (100%) |
| D1110 | Prophylaxis – Adult | Preventive | Class I (100%) |
| D1120 | Prophylaxis – Child | Preventive | Class I (100%) |
| D1206 | Fluoride Varnish Application | Preventive | Class I (100%) |
| D1351 | Sealant – Per Tooth | Preventive | Class I (100%) |
| D2140 | Amalgam Restoration, 1-surface | Restorative | Class II (80%) |
| D2330 | Composite Restoration, 1-surface, Anterior | Restorative | Class II (80%) |
| D2391 | Composite Restoration, 1-surface, Posterior | Restorative | Class II (80%) |
| D2740 | Crown – Porcelain/Ceramic | Restorative | Class III (50%) |
| D2750 | Crown – Porcelain Fused to High Noble Metal | Restorative | Class III (50%) |
| D2950 | Core Buildup, Including Any Pins | Restorative | Class II or III |
| D3310 | Root Canal – Anterior | Endodontic | Class II (80%) |
| D3330 | Root Canal – Molar | Endodontic | Class II (80%) |
| D4341 | Periodontal Scaling and Root Planing, 4+ teeth per quad | Periodontic | Class II (80%) |
| D4910 | Periodontal Maintenance | Periodontic | Class II (80%) |
| D5110 | Complete Denture – Maxillary | Prosthodontic | Class III (50%) |
| D7140 | Simple Extraction | Oral Surgery | Class II (80%) |
| D7210 | Surgical Extraction | Oral Surgery | Class II (80%) |
| D9940 | Occlusal Guard | Adjunctive | Class III or Not Covered |
Special Considerations for Major Procedures
Major dental procedures carry the highest costs and the greatest need for careful code verification. Let’s examine the coding landscape for crowns, bridges, implants, and dentures in greater detail.
Crown Coding Nuances
A crown recommendation triggers a cascade of decisions that affect the codes on your treatment plan. The dentist must determine the crown material, whether a buildup is necessary, and whether the tooth requires a root canal first. Each decision adds a potential code.
The crown material codes (D2740, D2750, D2790, and others) describe the final restoration. Your dentist will discuss material options with you. A fully ceramic crown (D2740) provides the best aesthetics for front teeth. A porcelain-fused-to-metal crown (D2750) offers a balance of strength and appearance for back teeth. A full gold crown (D2790) delivers maximum durability for patients who grind heavily. Your insurance plan may only cover a basic crown material, requiring you to pay the difference for upgraded materials, even if your plan otherwise covers crowns at 50%.
When a tooth is severely broken down, a core buildup (D2950) restores missing structure before the crown preparation. Some insurance companies consider a buildup to be incidental to the crown and will not pay separately. Your dental office should inform you before the procedure if a buildup is necessary and whether your insurance is likely to cover it. If insurance denies the buildup, you may owe the buildup fee even though the crown itself was covered.
Bridge Coding Structure
A bridge replaces one or more missing teeth by using adjacent teeth as anchors. The coding for a bridge appears as multiple line items because each component codes separately. A three-unit bridge replacing tooth 19, with retainers on teeth 18 and 20, generates the following codes: a retainer crown on tooth 18, a pontic for tooth 19, and a retainer crown on tooth 20. Each line item carries its own fee.
The material codes for retainers and pontics must match. You cannot have a porcelain retainer on one end and a gold retainer on the other. The pontic code describes the false tooth suspended between the retainers. Pontic codes include D6240 for a porcelain fused to high noble metal pontic and D6245 for a porcelain/ceramic pontic.
The “missing tooth clause” applies frequently to bridges. If tooth 19 was missing before your dental insurance coverage began, the insurance company may deny the pontic code. They might still cover the retainer crowns if those teeth need crowns for reasons unrelated to the bridge. This creates a situation where you pay for the pontic entirely out of pocket.
Implant Coding Breakdown
Dental implants have transformed tooth replacement, but their coding is fragmented. A single implant restoration involves multiple procedures with separate codes that may be performed over several months:
- The surgical placement of the implant body (D6010). This code covers the insertion of the titanium post into the jawbone.
- A second-stage surgery to expose the implant (D6011), sometimes necessary if the implant was buried under the gum during healing.
- The abutment placement (D6056), which attaches a connector to the implant body.
- The implant-supported crown (D6058 or D6059), which is the visible tooth portion.
Insurance coverage for implants varies dramatically. Some modern plans cover implants similarly to bridges. Many older or less expensive plans exclude implants entirely or provide only a token benefit equal to the cost of a partial denture. Before beginning implant treatment, obtain a pre-authorization that lists every anticipated code. Understand exactly what your plan will pay for each component. The total out-of-pocket cost for a single implant can range from $1,500 to $6,000 depending on your location and specific treatment needs.
The Future of Dental Procedure Coding
Dental coding continues to evolve. Several trends are shaping the future of the CDT Code and how it affects your experience as a patient.
Teledentistry Codes
The COVID-19 pandemic accelerated the adoption of virtual dental consultations. The CDT Code responded with teledentistry codes. A synchronous teledentistry visit (D9995) involves real-time audio and video communication between patient and provider. An asynchronous visit (D9996) involves the transmission of recorded information, such as photographs, for review by the dentist at a later time. These codes allow dentists to triage emergencies, monitor treatment progress, and conduct initial consultations without an in-person visit. Insurance coverage for teledentistry varies widely but is expanding.
Integration with Medical Coding
The boundary between dental and medical care blurs in certain clinical situations. Sleep apnea treatment with oral appliances, temporomandibular joint (TMJ) therapy, and treatment for traumatic injuries often cross the medical-dental divide. Future code development may include more codes that facilitate medical billing for conditions traditionally managed by dentists. This integration could expand coverage for patients whose medical plans provide better benefits than their dental plans.
AI and Automated Coding
Artificial intelligence is entering the dental revenue cycle. Software systems can now analyze clinical notes and radiographs to suggest appropriate CDT codes. These systems aim to reduce coding errors and improve consistency. For patients, AI-assisted coding could mean fewer claim denials due to code selection errors. However, the human element remains essential. A dentist’s clinical judgment about what constitutes a D4341 versus a D1110 cannot be fully automated.
Value-Based Care and Outcome Codes
The healthcare system is slowly shifting from fee-for-service payment to value-based payment that rewards positive patient outcomes. The CDT Code currently describes procedures performed, not outcomes achieved. Future code additions might include codes that track clinical results, allowing payment models that incentivize long-term health rather than procedural volume. This evolution could align financial incentives with your interest in maintaining oral health rather than receiving repeated treatment.
Building Your Personal Dental Code Reference Card
You do not need to memorize hundreds of codes. A handful of codes will cover the vast majority of your dental experiences. Create a personal reference card with the codes most relevant to your oral health history and keep it accessible. This card becomes a powerful tool during dental visits and insurance calls.
Start by reviewing your last three years of dental treatment. Identify the codes that appear repeatedly. List them with their official nomenclature and a brief note about what they mean in plain English. Add codes for any procedures your dentist has mentioned you might need in the future. Update this card annually when your insurance plan renews and the CDT Code updates.
Here is a template for a personal dental code reference card:
My Dental Codes Reference
- My Plan’s Annual Maximum: [Amount]
- My Deductible: [Amount]
- Class I Coverage (Diagnostic/Preventive): [Percentage]
- Class II Coverage (Basic Restorative): [Percentage]
- Class III Coverage (Major): [Percentage]
Frequent Codes:
- D0120 – Periodic Exam (routine checkup)
- D0272 – Bitewing X-rays (cavity detection)
- D1110 – Adult Cleaning (healthy gums)
- D2391 – White Filling, Back Tooth
Anticipated Codes:
- [List any procedures your dentist says you may need]
Questions for Insurance Calls:
- “What is the coverage percentage for code [XXXX] on tooth [number]?”
- “Have I met my deductible for this year?”
- “How much of my annual maximum remains?”
- “Are there any frequency limitations on this code?”
Carrying this card transforms phone calls with your insurance company from vague and frustrating to specific and productive. You become the informed patient that the system is designed to serve but rarely encounters.
Common Mistakes to Avoid When Reviewing Dental Codes
Patients who are new to navigating dental codes often make predictable mistakes. Learning about these pitfalls in advance helps you avoid them.
Assuming All Cleanings Are the Same
Many patients believe a “cleaning is a cleaning.” This assumption leads to the most frequent billing disappointment. A preventive cleaning (D1110) and a periodontal maintenance cleaning (D4910) are clinically and financially different. If you have a history of periodontal disease, you likely need D4910 for life. Insurance may cover D4910 differently than D1110. Confirm your specific code before each cleaning appointment, especially if you have changed dental offices.
Ignoring the Annual Maximum
Dental insurance plans cap their annual payout. If your plan has a $1,500 maximum and you have already used $1,200, your remaining benefit for the year is $300 regardless of your coverage percentages. Track your remaining maximum throughout the year. When possible, schedule major treatment across two calendar years to access two annual maximums. A treatment plan costing $3,000 split between December and January could result in $3,000 in insurance payments rather than $1,500.
Failing to Get a Pre-Authorization
Pre-authorizations take time and require effort from your dental office. Some patients skip this step to avoid delays. This choice saves a few weeks but risks significant financial exposure. For any procedure expected to cost more than a few hundred dollars out of pocket, insist on a pre-authorization. The written estimate from your insurance company provides a reliable basis for financial planning and gives you leverage if the actual payment falls short.
Not Understanding In-Network vs. Out-of-Network Rules
Your insurance plan negotiates lower fees with in-network dentists. If you visit an out-of-network dentist, the allowed amount may be lower than the dentist’s fee, and you pay the difference. Additionally, your plan might have higher coverage percentages for in-network care. Verify your dentist’s network status annually. Practices join and leave networks, and your favorite dentist might not be in-network with your current plan even if they were in-network last year.
Accepting Verbal Estimates Without Documentation
A front desk staff member saying “Your insurance will probably cover 80% of that” provides no protection. Get the estimate in writing on a treatment plan with codes. Follow up with your insurance company directly. Document the name of the representative you spoke with and the reference number for the call. If the insurance company later pays less than quoted, you have a record to support an appeal.
Teaching Your Family About Dental Codes
Dental literacy is a skill that benefits every member of your household. Teaching your children, your partner, or your aging parents about dental codes empowers them to navigate their own care effectively.
For children, keep the education simple and visual. Show them a treatment plan and point out the codes. Explain that D1120 is their special cleaning code. Teach them that D1206 is the fluoride that protects their teeth. When children understand that codes represent specific services, they begin to see dental visits as transparent and manageable. This early literacy reduces dental anxiety and builds a foundation for lifelong health advocacy.
For aging parents, focus on the codes most relevant to geriatric dental care. Complete dentures (D5110, D5120), periodontal maintenance (D4910), and extractions (D7140, D7210) become more common with age. Help your parents maintain a list of their current dental codes and understand their insurance coverage. Attend appointments with them if possible. Ask questions about the codes on their treatment plans. Your presence adds a layer of accountability that protects them from overtreatment or billing errors.
For your partner or spouse, coordinate your dental benefits if you have dual coverage. One of you might have coverage through your employer and the other through theirs. Understand the coordination of benefits rules that determine which plan pays first. The primary plan processes the claim and pays its share. The secondary plan then processes the remaining balance and may cover some or all of the patient portion. Providing both insurance cards to your dental office ensures proper claim submission and maximizes your combined benefits.
Resources for Verifying CDT Codes
You have access to several authoritative resources for confirming the meaning and validity of dental procedure codes.
The ADA CDT Manual: The American Dental Association publishes the complete CDT manual annually. This book contains every valid code, nomenclature, and descriptor. You can purchase the manual from the ADA store or access it through some public libraries. The manual is the definitive source. If a code appears in the CDT manual, it is legitimate. If it does not, it is not a valid dental procedure code.
Your Insurance Company’s Online Portal: Most dental insurance companies provide online access to plan documents, including the fee schedule for common codes. Log in to your portal and search for “fee schedule” or “covered services.” Some plans list covered codes with their associated patient copayment amounts, making financial planning straightforward.
State Dental Associations: Many state dental associations publish consumer resources that explain common codes and what patients should expect. These resources are usually free and written in accessible language. Search for your state’s dental association website and look for a “for the public” or “patient resources” section.
ADA Consumer Resources: The ADA’s public website, MouthHealthy.org, provides patient-facing information about dental procedures. While it does not focus on codes specifically, it explains treatments in plain language, helping you connect code numbers to clinical realities.
Your Dental Office’s Treatment Coordinator: An ethical dental office employs staff who genuinely want you to understand your treatment plan. The treatment coordinator or office manager should be willing to explain each code, answer your questions, and provide written documentation. If your dental office resists your questions about codes, consider whether that office aligns with your values as a consumer.
Conclusion
The ADA Code of Dental Procedures is not a secret language designed to confuse you; it is a standardized system that brings clarity, accountability, and transparency to your dental care. By learning how these codes are structured, what they mean, and how they interact with your insurance coverage, you transform from a passive recipient of dental services into an active, informed participant in your oral health journey. This guide has equipped you with the knowledge to read treatment plans, question discrepancies, and advocate for fair billing with confidence.
Frequently Asked Questions
What is the difference between D1110 and D4910?
D1110 is an adult prophylaxis, or preventive cleaning, for patients with healthy gums and no history of periodontal disease. D4910 is periodontal maintenance, a therapeutic cleaning for patients who have been treated for gum disease and require ongoing care at more frequent intervals to prevent recurrence. If you have a history of periodontal treatment, D4910 is likely the appropriate code for your continuing care.
Can a dental office charge me for a code my insurance denies?
Yes. Your relationship is with the dental office, not the insurance company. You are ultimately responsible for the fees associated with your treatment. If your insurance denies a claim for a service you received, the dental office can bill you for the full fee. This is why pre-authorization and coverage verification before treatment are essential.
Why do I see multiple codes for one tooth on my treatment plan?
Complex treatment often involves multiple procedures on the same tooth. A tooth might need a buildup (D2950) to replace missing structure, a post and core (D2954) for additional retention, and a crown (D2740) for final restoration. Each procedure codes separately because each requires distinct clinical work. A reputable dental office explains why each code is necessary.
How often does the ADA update dental codes?
The ADA updates the CDT Code annually. New codes, revised nomenclature, and deleted codes take effect January 1 of each year. Dental offices must update their billing systems to reflect the current code set. If you receive treatment early in the year, confirm that your provider is using the current year’s codes.
What should I do if I suspect my dental office used the wrong code?
First, ask for clarification. Bring your concern to the office manager or treatment coordinator. Say, “I noticed this code on my bill, and after reading about it, I’m not sure it matches the treatment I received. Can you help me understand?” If the explanation is unsatisfactory and you still suspect incorrect coding, contact your insurance company’s fraud hotline or your state dental board. Intentional miscoding is fraud and should be reported.
Additional Resource:
For the most current and authoritative information, visit the American Dental Association’s official page on dental procedure codes: ADA Code on Dental Procedures and Nomenclature
Disclaimer:
This article provides general information about dental procedure codes for educational purposes only. It does not constitute medical, dental, or legal advice. Dental codes, insurance coverage, and treatment recommendations vary based on individual circumstances. Always consult with your treating dentist about your specific treatment needs and with your insurance company about your specific coverage. Code information was accurate as of the time of writing, but the ADA updates the CDT Code annually. Verify current codes with official sources before making decisions based on the information in this article.