what happens if tooth infection not treated
When a sharp pain in your tooth fades away, you might feel a wave of relief. Many people assume the problem has solved itself. This silent stage is often the most dangerous phase of a dental infection. Understanding what happens if tooth infection not treated goes far beyond saving a tooth. It is a matter of protecting your overall health and, in severe cases, your life.
A tooth infection, medically known as an odontogenic infection, is a bacterial invasion at the core of your tooth. It never heals on its own. Without professional intervention, the bacteria multiply, destroy surrounding tissues, and embark on a destructive journey through your body. This guide will walk you through every stage of this progression, from a simple cavity to rare but life-threatening complications. We will explore the science, the symptoms, and the critical timelines that demand immediate action.
Understanding the Anatomy of a Tooth Infection
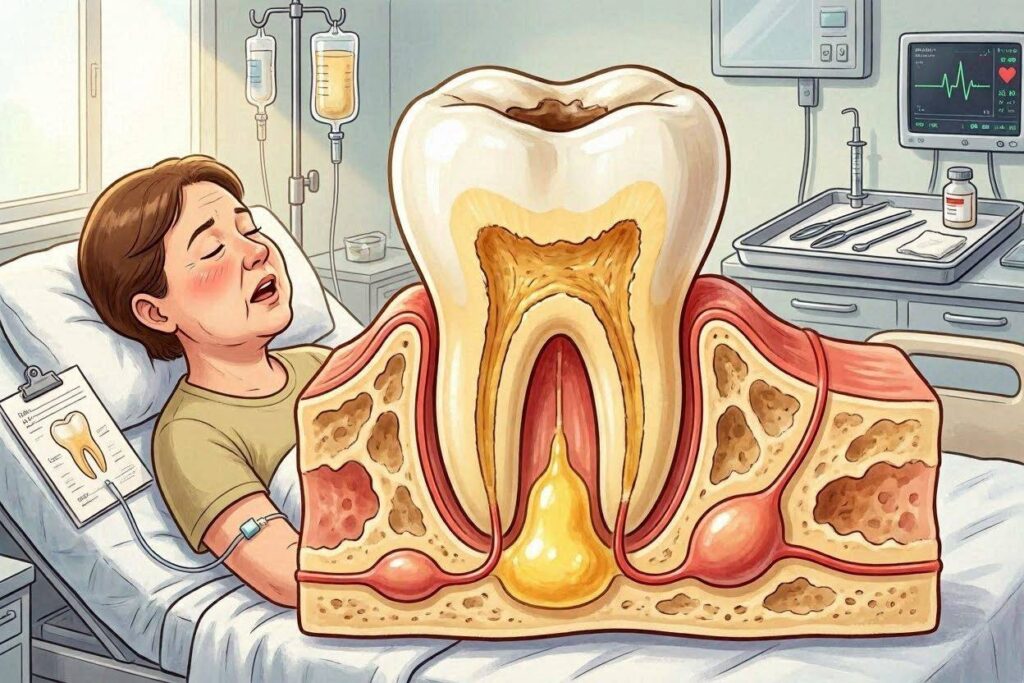
To grasp the danger, you must first understand the battlefield. A tooth is not a solid piece of bone. Beneath the hard, white enamel and the cementum layer lies a soft, living core called the pulp. This chamber houses blood vessels, nerves, and connective tissue. When decay, a crack, or trauma exposes this inner sanctum, bacteria flood in.
The pulp becomes inflamed, a condition known as pulpitis. Because the pulp sits inside rigid walls, the swelling has nowhere to go. Pressure builds, strangling the blood supply and killing the nerve. This is why a severe toothache can suddenly stop. The absence of pain does not signal recovery. It signals death. The dead tissue becomes a perfect breeding ground for bacteria. The infection then spills out from the root tip into the jawbone, establishing a periapical abscess.
Key Insight: A “silent” tooth with no pain can harbor an active, spreading infection visible only on an X-ray.
Stage One: The Initial Abscess and Localized Destruction
The first consequence of an untreated infection is an abscess. A dental abscess is a pocket of pus that forms at the root tip. Your immune system walls off the infection to prevent its spread, creating a painful, pressure-filled sac. The body’s reaction here is aggressive and localized.
Symptoms of a Localized Abscess
You will likely notice several distinct and uncomfortable signs:
- Intense, throbbing pain: The pain is persistent and often worsens when lying down.
- Sensitivity to temperature: Extreme reactions to hot or cold linger long after the stimulus is removed.
- Pain when chewing: Any pressure on the tooth causes sharp discomfort.
- Facial swelling: The gum and cheek near the tooth become red and puffy.
- Foul taste: If the abscess ruptures, a sudden rush of salty, bad-tasting fluid fills the mouth.
- A pimple on the gum: A small bump called a fistula appears. This is a drain tunnel for pus.
At this stage, the infection remains confined to the immediate area. The bone around the root tip begins to resorb. Dentists identify this on an X-ray as a dark halo, or radiolucency, at the root end. This is a granuloma or cyst. The bone literally dissolves to make room for the thriving bacteria. While the immune system holds the line, it cannot win the war. The bacteria inside the dead tooth remain protected from antibiotics and immune cells. The resolution requires a dentist to mechanically remove the infected pulp source, either through a root canal or extraction.
Stage Two: The Spread to Fascial Spaces
If you ignore the localized abscess, the pus seeks the path of least resistance. It breaks through the jawbone and enters the soft tissue planes of the face and neck, known as fascial spaces. This progression marks a critical escalation. The infection is no longer a dental problem. It is a surgical emergency.
Specific Facial Infections by Tooth Location
The tooth’s location dictates where the swelling travels, often distorting your appearance and threatening vital functions.
| Affected Tooth | Potential Space of Spread | Visible Signs and Dangers |
|---|---|---|
| Lower Molars | Submandibular, Buccal, or Sublingual spaces | Hard swelling under the jawline, pushing the tongue up. Severe trismus (lockjaw) occurs. |
| Upper Canines | Canine space | Obliterates the nasolabial fold, swelling extends to the eye. Risk of spread to the cavernous sinus. |
| Lower Wisdom Teeth | Submasseteric or Parapharyngeal spaces | Deep, hard swelling. Risk of airway compromise, difficulty swallowing (dysphagia). |
| Upper Molars | Buccal space, Maxillary sinus | Cheek swelling that can close the eye. Pus can drain into the sinus, causing chronic sinusitis. |
Once the infection occupies these spaces, facial swelling becomes grossly apparent. A person with an untreated lower molar infection might develop a swelling the size of a golf ball or larger under the jaw. The skin turns red, taut, and feverish to the touch. More perilous is the involvement of the muscles. The chewing muscles, masseter and pterygoids, often sit near these spaces. Irritation causes trismus, where muscle spasms limit mouth opening to just a few millimeters. This symptom alone signals a dangerous deep-space infection and complicates any attempt at an oral examination.
Serious Warning Sign: If you cannot open your mouth to fit two fingers stacked between your front teeth, you have severe trismus, a medical emergency.
Stage Three: Ludwig’s Angina – The Airway Threat
Among the most feared consequences of what happens if tooth infection not treated is Ludwig’s angina. This is not a typical angina related to the heart. It is a rapidly spreading, gangrenous cellulitis affecting the floor of the mouth, under the tongue, and the neck. It most often originates from an infected lower second or third molar.
Ludwig’s angina is terrifying because of its speed and its target: your ability to breathe. The infection does not form a single pocket of pus but dissects through soft tissues like a destructive veil.
The Hallmarks of Ludwig’s Angina
- Board-like swelling: The neck becomes hard, tense, and painfully swollen to the touch, not soft and fluid-filled.
- Elevated and protruding tongue: The tongue is forced up against the palate and eventually pushed backward toward the throat.
- Muffled or “hot potato” voice: The swelling alters the voice, making it sound thick and indistinct.
- Drooling and inability to swallow: The patient cannot manage their own saliva.
- Respiratory distress: As the airway narrows, stridor (a high-pitched, wheezing sound on inhalation) begins. This precedes complete airway closure.
In an emergency room, a diagnosis of Ludwig’s angina triggers an immediate response. Securing the airway is the absolute first priority. The swelling distorts the anatomy so drastically that intubation becomes exceedingly difficult. Physicians often require a fiber-optic scope and an awake tracheotomy as a final resort—a surgical incision directly into the windpipe. Without such aggressive measures, death from asphyxiation is a grim reality. The mortality rate in the modern era, with aggressive surgical and antibiotic therapy, still hovers around 4-8%. Untreated, it is universally fatal.
Stage Four: Systemic Invasion and Sepsis
The infection’s journey does not stop at the neck. Bacteria can erode into blood vessels, or the sheer number of organisms can overwhelm the fascial barriers. This releases a continuous shower of bacteria and their toxic byproducts into the bloodstream. The result is bacteremia, which can rapidly progress to sepsis.
Sepsis is a life-threatening organ dysfunction caused by a dysregulated host response to infection. Your body’s defense system turns against itself. The immune response, designed to kill bacteria, triggers massive inflammation everywhere. Blood vessels leak, circulation collapses, and organs fail.
The Sepsis Pathway from a Dental Source
- Bacteria Enter Blood: Streptococcus or Staphylococcus species from the abscess enter the circulation.
- Cytokine Storm: The immune system releases a flood of inflammatory mediators.
- Endothelial Damage: The lining of blood vessels is damaged, causing clots and leaks.
- Hypoperfusion: Blood pressure plummets, and the body diverts blood from organs to save the heart and brain.
- Organ Failure: Kidneys stop filtering, lungs fill with fluid (ARDS), and the liver fails.
Recognizing Sepsis in Adults
Public health campaigns often summarize the signs with the acronym SEPSIS:
- S – Slurred speech or confusion.
- E – Extreme shivering or muscle pain.
- P – Passing no urine in a day.
- S – Severe breathlessness.
- I – “I feel like I might die.”
- S – Skin mottled, discolored, or very pale.
A patient in septic shock from a tooth infection requires intensive care. They receive large volumes of intravenous fluids, powerful vasopressors to maintain blood pressure, and broad-spectrum IV antibiotics. Surgeons must also drain the primary source of infection without delay. Blood cultures in these cases frequently grow oral streptococci. The mortality rate for septic shock ranges from 30% to 50%, even with the best medical care. A toothache, left to fester, can quite literally poison your blood.
Stage Five: Distant Organ Seeding and Abscesses
Bacteria circulating in the blood do not only trigger a generalized inflammatory storm. They can dock and colonize in distant organs, establishing metastatic abscesses far from the original tooth. This is a rare but devastating complication of prolonged dental neglect.
The Brain Abscess
The brain has a special and dangerous relationship with dental infections. The brain’s blood-brain barrier usually protects it, but oral bacteria, particularly the Streptococcus anginosus group, possess a unique ability to invade and cause abscesses here. A 2023 meta-analysis in the Journal of Dentistry confirmed a strong link between poor oral health and brain abscesses. Often, these patients have no clear source of infection other than a silent dental problem.
Symptoms of a brain abscess are insidious. They include a persistent, dull headache that does not respond to usual painkillers. Focal neurological deficits appear, like weakness on one side of the body or vision changes. Seizures can occur without a prior history. Fever is often absent, making the diagnosis tricky. Treatment requires a long course of IV antibiotics and, often, a craniotomy to drain the pus. The consequences can be permanent cognitive impairment, paralysis, or death.
Endocarditis: The Heart Valve Infection
The heart’s inner lining, particularly its valves, is a prime target for blood-borne bacteria from a tooth infection. This condition is infective endocarditis. Bacteria settle on the heart valves, forming clumps of microorganisms and platelets called vegetations. These vegetations can destroy the valve itself.
The link is so strong that dental procedures are a classic cause of endocarditis in at-risk individuals. An untreated abscess provides a constant, high-dose bacterial drip directly from the tooth socket into the venous system. Symptoms include a new or changing heart murmur, persistent fevers, night sweats, and small, painless spots on the palms or soles called Janeway lesions. The destruction of the valve leads to acute heart failure. Treatment involves weeks of IV antibiotics. Severe cases require open-heart surgery to replace the destroyed, infected valve with a prosthetic one. The mortality rate for infective endocarditis is substantial, around 20% in-hospital.
Other Distant Infections
The lungs receive the entire venous return, making them a filter for septic emboli. A dental infection can cause aspiration pneumonia or lung abscesses. The kidneys can suffer from glomerulonephritis, where immune complexes, not just the bacteria, damage the delicate filtration units. Septic arthritis can occur if bacteria settle in a prosthetic knee or hip joint. In spinal health, there is a described correlation between chronic dental infections and discitis, an infection of the spinal disc space. The body’s constant, low-grade fight against a tooth infection also contributes to a state of chronic systemic inflammation, which leads us to long-term, silent damage.
The Chronic, Systemic Impact of Leaving Infection
The dramatic acute emergencies grab headlines, but the chronic, low-grade consequences of an untreated tooth infection exact a far wider toll on public health. The body’s constant immune response to a contained but still active infection pours inflammatory mediators into the bloodstream over months or years. This chronic inflammation is a slow poison.
The Cardiovascular Connection
The most robust evidence for systemic harm links periodontitis and chronic endodontic infections to heart disease. C-reactive protein (CRP), a key marker of inflammation and a predictor of heart attack risk, is elevated in people with chronic dental infections. The bacteria Porphyromonas gingivalis and others from the mouth can invade arterial walls. They accelerate the formation of atherosclerotic plaques, making them more prone to rupture and cause a heart attack or stroke.
A major study published in the Journal of Dental Research found that untreated apical periodontitis—the dental term for the chronic infection at a tooth root—was independently associated with an increased risk of cardiovascular disease, even after adjusting for classic risk factors like smoking and diabetes. The inflammation is the bridge. Removing the infected tooth or performing a root canal resolves the local inflammation and has been shown to lower systemic inflammatory markers.
The Diabetes Connection
A dangerous two-way relationship exists between diabetes and tooth infections. High blood sugar provides a rich food source for bacteria and impairs the immune system, making severe, rapidly spreading infections more likely. A diabetic patient with an untreated tooth infection is a setup for a crisis.
Conversely, a chronic infection makes diabetes much harder to control. The inflammatory mediators released during the fight against the infection actively increase insulin resistance. The body’s cells do not respond to insulin properly, causing blood sugar to rise. This frustrating cycle often sees patients’ glucose levels dramatically improve once a chronic dental infection is eliminated. In diabetic management, dental clearance is not optional; it is a primary therapeutic measure.
The Pregnancy Risk
Pregnancy places the body in a naturally immunocompromised state. A dental infection during pregnancy is not a small inconvenience. It is a significant risk to both mother and child. The bacteria and inflammatory toxins can cross the placental barrier.
Research links maternal periodontal disease and chronic infections to preterm birth, low birth weight, and preeclampsia. The proposed mechanism is that oral pathogens reach the uterus and cause inflammation, triggering premature labor. The acute pain and systemic stress of a full-blown abscess can also pose a direct threat to the pregnancy. The second trimester is the safest window for dental treatment. A tooth infection, however, is an emergency at any stage of pregnancy, and aggressive, safe treatment with local anesthesia and pregnancy-safe antibiotics is the standard of care, as the risk of non-treatment far outweighs the procedural risk.
A Dangerous Misconception: The “Natural Cure” Fallacy
The internet is filled with dangerous advice on how to “cure” a tooth infection without a dentist. Common, dangerous recommendations include oil pulling, applying garlic or a crushed aspirin tablet directly to the gum, and taking large doses of various herbs. These methods will not cure a true tooth infection.
The core problem is the dead or necrotic pulp tissue inside the tooth. This internal space has no blood supply left. An antibiotic, whether oral or intravenous, cannot penetrate there. A herbal poultice certainly cannot. The bacteria thrive in this protected, non-living cavern. A pimple on the gum can be drained, but the factory producing the pus remains intact, high up inside the tooth roots. The only cure is the physical removal of the source. A dentist does this by cleaning, shaping, and sealing the canal system (a root canal) or by removing the entire tooth (extraction). Believing in “natural cures” simply buys time for the bacteria to spread deeper, turning a simple procedure into a surgical emergency.
The Definitive Treatment Pathway: What to Expect
Facing a tooth infection is stressful, but understanding the clear, step-by-step treatment path removes the fear of the unknown. Modern dentistry makes this process predictable and comfortable.
Diagnosis: The Critical First Step
The dentist begins with a thorough history. They listen to the symptoms, the timeline, and the character of the pain. A clinical exam follows, including tapping on the tooth. A sharp pain on percussion is a cardinal sign of a periapical infection. They test the nerve’s vitality with a cold spray. A dead tooth will not feel the cold. A healthy tooth will feel a quick, sharp sensation that goes away.
An X-ray, typically a periapical radiograph, provides the definitive image. The infection appears as a dark spot at the end of the root. A Cone Beam Computed Tomography (CBCT) scan, a 3D X-ray, offers a far more detailed view, showing the exact size of the bone lesion and its proximity to critical structures like the maxillary sinus or the inferior alveolar nerve. This technology has revolutionized the diagnosis and treatment of complex infections.
Treatment Decision: Root Canal vs. Extraction
This is the central choice. The goal is always to save the tooth when possible.
| Feature | Root Canal Treatment (Endodontics) | Tooth Extraction |
|---|---|---|
| Goal | Remove the infection and save the natural tooth. | Remove the entire infected tooth. |
| Procedure | The infected pulp is removed. The canals are cleaned, disinfected, and sealed. A crown is usually needed later. | The tooth is loosened and removed. The socket is cleaned. |
| Pain During | Completely painless with modern local anesthesia. | Completely painless with modern local anesthesia. |
| Recovery | Minimal post-op sensitivity for a few days. | Slightly more intense short-term healing pain as the socket closes. |
| Long-term | Maintains natural function, bite, and prevents bone loss. High success rate. | Leaves a space that requires replacement (implant, bridge) to prevent shifting and further bone loss. Higher long-term cost and complexity. |
| When Preferred | Tooth has a good prognosis, adequate crown structure, and strategic importance. | Tooth is cracked vertically, has a hopelessly decayed root, or severe bone loss. Can be a choice for wisdom teeth. |
An abscess does not always require an immediate, full root canal in one visit. Many dentists perform a pulpectomy, removing the bulk of the infected nerve and placing a sedative medicament inside the tooth to calm the acute infection before completing the procedure at a second visit. Antibiotics are an adjunct, not a primary treatment. They are prescribed only when signs of systemic spread exist, like fever, significant swelling, or trismus. For a simple localized abscess without swelling, antibiotics are often not needed.
Critical Note: Never demand antibiotics from a dentist for a toothache without an exam. Misuse only fuels antibiotic resistance, and the pill will not reach the dead pulp to kill the source of the infection.
The High Cost of Delay: A Financial and Emotional Toll
Delaying treatment for a tooth infection transforms a predictable, low-cost procedure into a catastrophic health crisis with life-altering financial implications.
A Cost Comparison Table:
| Treatment Scenario | Average Cost Range (Illustrative) | Time Investment |
|---|---|---|
| Immediate Care | ||
| Exam & X-ray | $150 – $350 | 1 hour |
| Root Canal (Molar) & Crown | $3,000 – $4,500 | 2-3 visits |
| Delayed Care (Local Spread) | ||
| Incision & Drainage | $500 – $1,500 | Emergency visit |
| Root Canal & Crown | $3,000 – $4,500 | 3-4 visits |
| Delayed Care (Systemic/Sepsis) | ||
| ER Visit, CT Scan | $5,000 – $10,000+ | 3-5 hours |
| Hospitalization (1-5 days) | $2,000 – $10,000+ per day | 1-5 days |
| Surgical Draining, IV Antibiotics | $15,000 – $50,000+ | 5-10 days |
| Total Cost of Delay | Can exceed $80,000 | Weeks of lost work |
This table does not capture the emotional cost. The days lost from work, the trauma of an ICU stay, the scarring from surgical drainage, and the possible permanent disfigurement or nerve damage. The chronic pain endured before the acute event erodes the quality of life, sleep, and mood. A problem that is quiet, contained, and fixable for a few hundred dollars becomes a bankruptcy-level medical event that steals months of health.
A Special Note on Antibiotics: A Double-Edged Sword
A dedicated section on antibiotics is essential because their role is widely misunderstood. Patients often demand a prescription, believing it will cure their dental infection. It will not. As stressed earlier, the source of infection is a space inside the tooth without blood flow. Oral antibiotics cannot reach the bacteria living there. They only control the infection in the surrounding tissues.
The prescription of antibiotics for a dental emergency is a decision made solely on the presence of systemic signs or a rapidly spreading facial cellulitis. Dentists follow strict prescribing guidelines to combat the global crisis of antibiotic resistance. A dentist may prescribe Penicillin VK or Amoxicillin as the first line. For those allergic, Clindamycin or Azithromycin are common alternatives. The most terrifying consequence of antibiotic misuse is a Clostridium difficile (C. diff) infection, a severe, debilitating colitis. An untreated tooth infection is dangerous. Resorting to un-prescribed or “leftover” antibiotics without treating the tooth’s source adds this severe risk with zero chance of a cure.
Prevention: The Undisputed Answer
The entire cascade of pathology, from a pinprick cavity to Ludwig’s angina, is nearly 100% preventable. The conversation is incomplete without a clear, actionable framework for prevention.
- Non-Negotiable Oral Hygiene:
- Brush twice daily with a soft-bristled brush and fluoride toothpaste. Aim for two minutes.
- Floss or use interdental brushes once daily. The toothbrush does not reach the spaces where most infections begin.
- Dietary Discipline:
- Sugar is the primary enemy. Bacteria metabolize free sugars to produce the acid that demineralizes teeth. Limit the frequency of sugar intake, not just the quantity. Sipping a soda over two hours is more damaging than drinking it quickly.
- Rinse with water after consuming sugary or acidic foods.
- Regular Professional Check-ups:
- A 6-month recall is the standard. A dentist can detect a small cavity before it reaches the pulp. A small filling is a trivial procedure. A 12-month interval might miss the rapid progression of decay.
- Early Intervention:
- Never ignore a small chip, a rough edge, or mild cold sensitivity. These are warning whispers. Addressing a cavity early avoids the eventual, inevitable crisis.
Frequently Asked Questions
Can a tooth infection go away on its own?
No. A tooth infection inside a dead nerve space will never self-resolve. The pain may vanish when the nerve dies, but the bacterial source and the abscess in the bone persist and silently expand.
What are the first signs of sepsis from a tooth infection?
Be vigilant for a combination of high fever or abnormally low body temperature, rapid heartbeat, lightheadedness or feeling faint, confusion, and mottled or pale skin. This is a 911-level emergency.
Is a gum abscess the same as a tooth abscess?
No. A gum (periodontal) abscess starts in the gum pocket. A tooth (periapical) abscess starts at the root tip from a dead nerve. A tooth abscess can drain through the gum, appearing like a “gum boil,” but the origin is the tooth itself.
How long can you have a tooth infection before it kills you?
There is no set timeline. Sepsis can develop in hours, while a chronic abscess can smolder for years before a sudden, catastrophic flare-up. Any delay is a gamble with no safe period.
Can a tooth infection affect your brain?
Yes. Oral bacteria, particularly the Streptococcus anginosus group, can travel through the bloodstream and cause a life-threatening brain abscess. A severe, persistent headache with a known dental infection requires an immediate emergency room visit.
Additional Resource:
For detailed, evidence-based information on sepsis symptoms, visit the official resource of the Sepsis Alliance at www.sepsis.org. This organization provides clear, life-saving tools for recognizing this medical emergency early.
Conclusion
An untreated tooth infection is a ticking time bomb, transitioning from a localized cavity to a life-threatening systemic crisis like sepsis or a brain abscess. The silent destruction erodes your jawbone, strains your heart, and can close off your airway without warning. Remember, a dead tooth can never heal itself; the only safe and effective path is to break the cycle of fear and seek immediate professional dental care to remove the source of infection definitively.
Disclaimer: This article is for informational purposes only and does not constitute professional medical or dental advice. If you suspect you have a dental infection, seek immediate evaluation from a licensed dentist or medical provider. In cases of breathing difficulty or severe systemic symptoms, call emergency services immediately.



