What Is A Dental Implant Arch?
Living with a failing smile reshapes your daily life in ways others rarely understand. You might catch yourself hiding your mouth when you laugh at a colleague’s joke. You might refuse the steak your partner grilled perfectly. You might study old photographs and grieve a version of yourself that seemed so effortless.
Modern dentistry offers a way back. Not the temporary, compromised return that removable dentures provide, but a genuine restoration of function, confidence, and identity. The solution sits at the intersection of surgical precision and prosthetic artistry. Dentists call it a dental implant arch.
This guide walks you through everything you need to know about this life-changing treatment. We will cover the anatomy, the procedure, the investment, the recovery, and the realistic outcomes. No sensational promises. No watered-down explanations. Just honest, thorough information from someone who understands that knowledge reduces fear.
Take your time with this article. It runs long because the topic deserves depth. By the end, you will possess a clear, realistic understanding of what a dental implant arch is and whether it might represent your path back to a complete smile.
Understanding the Dental Implant Arch: More Than Just “New Teeth”
Dental terminology often confuses patients. Marketing teams coin buzzwords. Clinics trademark proprietary names. You read about All-on-4, Teeth-in-a-Day, fixed hybrid dentures, and full-arch implant bridges. Beneath the branding, the core concept remains consistent and beautifully logical.
A Precise Definition
A dental implant arch is a complete row of prosthetic teeth—either upper, lower, or both—fixed permanently to a strategic number of dental implants surgically placed in the jawbone. Unlike traditional dentures that rest on your gums and come out at night, an implant arch stays in your mouth 24 hours a day, 7 days a week. Only your dentist can remove it for maintenance.
Think of an arch as a bridge that replaces every tooth on one jaw. Natural teeth are anchored by roots embedded in bone. A dental implant arch replaces those roots with titanium or ceramic posts and crowns the visible portion with lifelike prosthetic teeth. The result mimics nature’s engineering so closely that many patients report forgetting they ever lost teeth in the first place.
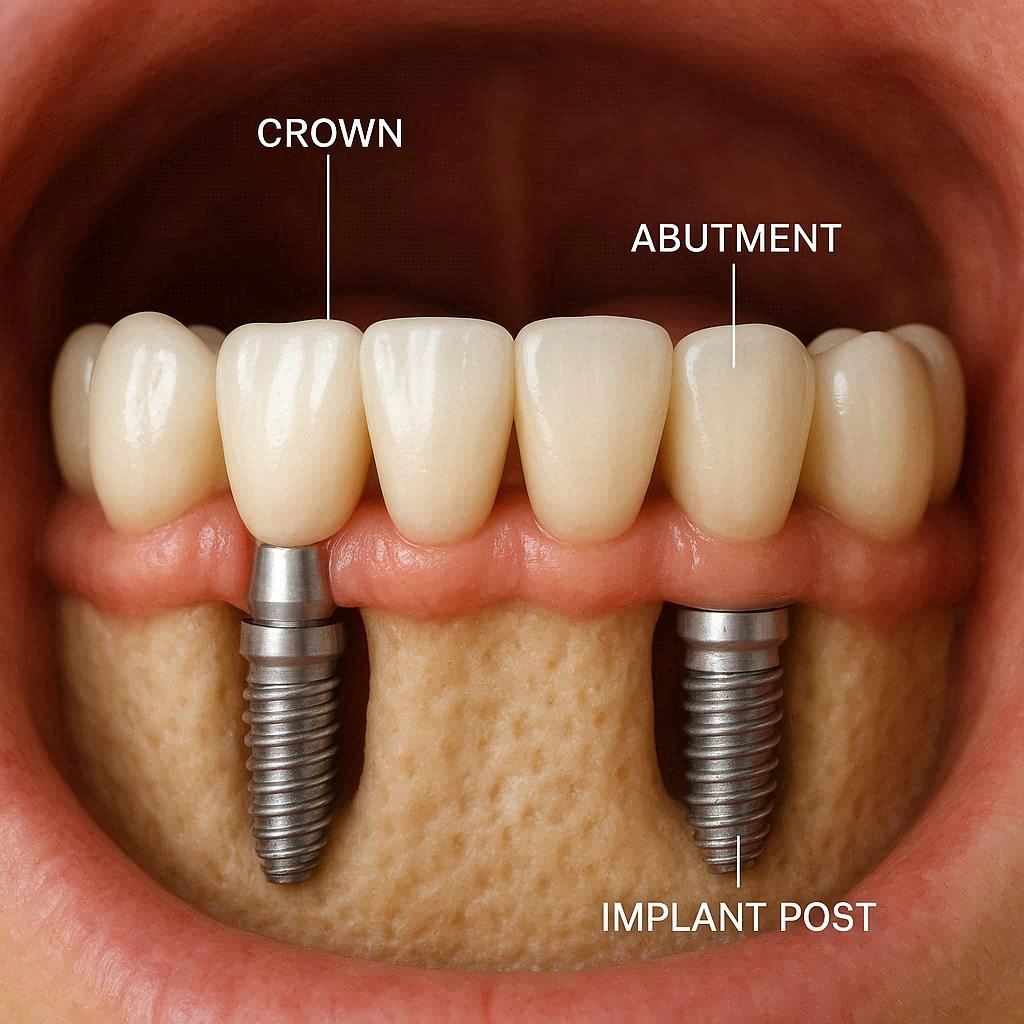
The Components of an Implant Arch
Every dental implant arch consists of three fundamental layers. Understanding these layers helps you make informed decisions about materials, costs, and long-term maintenance.
The Implant Fixtures
The deepest layer. These screw-shaped posts, typically made from biocompatible titanium or zirconia, integrate directly with your jawbone through a process called osseointegration. They serve as artificial tooth roots. For a full arch, dentists usually place between four and eight implants per jaw. The exact number depends on your bone volume, bone density, and the specific treatment protocol your surgeon selects.
The Abutments
The middle connectors. Abutments attach to the implant fixtures and protrude through the gum tissue. They create a stable platform onto which the prosthetic arch fastens. Some systems use multi-unit abutments, which offer flexibility in angulation. Others use stock or custom abutments fabricated from titanium or zirconia.
The Prosthetic Arch
The visible layer. This horseshoe-shaped restoration carries anywhere from ten to fourteen artificial teeth set in a gum-colored acrylic or composite base. High-end restorations may use a milled titanium bar wrapped in acrylic, a monolithic zirconia framework, or a hybrid design. The prosthetic replaces both your clinical crowns and a portion of the gum tissue lost to resorption.
How an Implant Arch Differs from Other Restorations
Patients often begin their research assuming all tooth replacement options are variations of the same idea. They are not. The differences matter significantly for your day-to-day experience.
Implant Arch vs. Traditional Dentures
Traditional dentures rely on suction, adhesives, and the underlying gum ridge for stability. They move when you speak. They shift when you chew. They require removal every night. A dental implant arch eliminates all of these compromises. The implants lock the restoration in place. You do not remove it. You do not apply adhesive. You simply live your life.
Implant Arch vs. Implant-Retained Overdentures
Overdentures clip onto a few implants but still come out for cleaning. They offer more stability than conventional dentures but less than a fixed arch. Patients who choose overdentures often do so for budget reasons or because they lack bone volume for a fully fixed solution. A fixed implant arch, by contrast, stays in the mouth permanently and feels more like natural teeth.
Implant Arch vs. Individual Implant Crowns
Replacing every missing tooth with an individual implant and crown would require placing twelve or more implants per arch. The cost and surgical burden make this approach impractical for most fully edentulous patients. The implant arch elegantly solves this problem by distributing chewing forces across fewer implants connected by a rigid framework.
| Feature | Traditional Dentures | Implant Overdentures | Fixed Implant Arch | Individual Implant Crowns |
|---|---|---|---|---|
| Stability | Low; moves during eating and speaking | Moderate; clips onto 2-4 implants | High; fixed to 4-8 implants | Very high; each tooth on its own implant |
| Removability | Patient removes daily | Patient removes for cleaning | Dentist removes only | Cannot be removed |
| Bone Preservation | None; accelerates resorption | Some stimulation from implants | Significant stimulation from implants | Maximum stimulation |
| Cost per Arch | $1,500 – $4,000 | $10,000 – $25,000 | $20,000 – $45,000 | $50,000 – $90,000+ |
| Treatment Time | 2-6 weeks | 3-6 months | 4-8 months (conventional) | 6-12 months |
| Palatal Coverage | Full coverage for uppers | Some coverage possible | No coverage; open palate | No coverage |
Important Note: Costs vary dramatically by geographic region, surgeon experience, and materials selected. The figures above represent reasonable ranges in the United States as of 2026. Always obtain multiple consultations and itemized treatment plans.
Why Patients Pursue an Implant Arch: The Unspoken Motivations
Clinical bullet points list indications like “edentulism” and “severe periodontal disease.” Those words sanitize the human experience driving patients into treatment. Understanding the real motivations matters because your own reasons shape your expectations and satisfaction.
The Functional Collapse
Teeth fail progressively for most people. You lose one molar and compensate by chewing on the other side. Then another fails. Then the remaining teeth drift, tip, and wear abnormally. By the time patients consider a full arch restoration, many have spent years navigating what dentists call “dental crippling”—a state where normal chewing becomes impossible.
They order only soft foods. They cut everything into tiny pieces. They avoid social meals entirely. One patient described attending her daughter’s wedding reception and spending the entire dinner pushing food around her plate, terrified her partial denture would dislodge mid-bite. She never tasted the $85 filet mignon.
A properly executed implant arch restores approximately 90% of natural chewing capacity. Compare that to traditional dentures, which recover perhaps 20-30%. You eat what you want. You bite into an apple. You chew a medium-rare steak. The simple pleasures return.
The Aesthetic Erosion
Bone resorption following tooth loss follows a predictable and unforgiving pattern. Without roots stimulating the alveolar bone, the body resorbs that structure. The jaw shrinks. Facial height collapses. Lips invert. Wrinkles deepen around the mouth. Patients develop what prosthodontists call “denture face”—the prematurely aged appearance associated with long-term tooth loss.
A dental implant arch does more than replace teeth. It restores facial support. The prosthetic base fills out the lip profile. The implants preserve remaining bone and slow further resorption. Patients who receive implant arches often appear younger afterward. Not because the teeth look unnatural or “too perfect,” but because proper facial proportions return.
The Psychological Toll
We underestimate the psychological weight of tooth loss until we listen to patients describe it. Embarrassment. Shame. A sense of crumbling identity. Denture wearers report constant anxiety about their prostheses clicking, slipping, or falling out during conversation. They stop smiling for photographs. They cover their mouths when they laugh.
Dental implant arches liberate patients from this psychological burden. The restoration stays fixed. You forget about it in the same way you forgot about healthy natural teeth—they simply work. Patients report dramatic improvements in quality of life scores, self-esteem metrics, and social engagement after treatment.
“I didn’t realize how much mental energy I spent worrying about my dentures until I didn’t have to anymore. The implant arch gave me back my spontaneity.” — Patient testimonial, 62-year-old female, full upper arch restoration
Medical Implications
Tooth loss correlates with systemic health decline. Patients with significant tooth loss consume fewer nutrient-dense foods. They favor processed carbohydrates over fresh vegetables, lean proteins, and fiber-rich fruits. Nutritional deficiencies compound over time.
Furthermore, chronic low-grade inflammation from failing dentition contributes to cardiovascular risk, poor glycemic control in diabetics, and cognitive decline associations in some studies. Restoring functional dentition allows patients to return to a whole-food diet. The medical benefits extend far beyond the mouth.
The Surgical Foundations: How Implant Arches Actually Work
Understanding the biomechanics behind implant arches gives you a deeper appreciation for why this treatment succeeds so predictably. The concepts are not particularly complicated, but they rarely receive adequate explanation.
Osseointegration: The Biological Miracle
In the 1950s, a Swedish orthopedic surgeon named Per-Ingvar Brånemark discovered something remarkable while studying blood flow in rabbit bone. Titanium chambers he implanted became so thoroughly integrated with the surrounding bone that he could not remove them without fracturing the bone itself. He named this phenomenon osseointegration.
Modern dental implants exploit this same biological process. A titanium or zirconia implant, placed precisely into prepared bone, triggers a healing response. Osteoblasts—bone-forming cells—migrate to the implant surface and begin depositing new bone directly onto the microscopically roughened surface. Within three to six months, the implant and bone form a structural and functional unit.
No synthetic material ever fully replaces a natural periodontal ligament, the shock-absorbing connective tissue around natural teeth. But osseointegrated implants approximate natural tooth anchorage remarkably well. The bone remodels continuously in response to loading, just as it does around natural roots.
Load Distribution Through the Arch Form
A single implant supporting a single molar crown experiences concentrated forces during chewing. The implant, surrounding bone, and prosthetic components must withstand these localized loads. When you replace an entire arch, however, you connect multiple implants with a rigid framework. This splinting effect fundamentally changes the biomechanics.
Forces applied during chewing distribute across all the implants and the entire prosthetic arch. A bite force that might overload one implant instead divides among four, six, or eight fixtures. The arch form itself—the curve of the prosthesis—provides mechanical advantage. Think of a Roman arch bridge: individual stones would collapse under load, but properly arranged and connected, they support enormous weight.
This principle explains why surgeons can restore an entire arch on as few as four implants. The implants do not correspond one-to-one with teeth. Instead, they act as a team. The prosthetic arch serves as the unifying structure.
Angulation Strategies: The All-on-4 Concept
The All-on-4 treatment concept, developed by Portuguese dentist Dr. Paulo Malo in the 1990s, revolutionized full-arch implantology. The insight was elegant: by tilting the posterior implants at an angle of 30 to 45 degrees, surgeons could place longer implants while avoiding the maxillary sinuses in the upper jaw and the inferior alveolar nerve in the lower jaw.
Angled placement offers several advantages:
- Longer implants engage more bone, increasing primary stability
- The tilted fixtures often anchor in denser bone anterior to the sinus cavities
- Angled multi-unit abutments correct the prosthetic emergence, allowing the prosthetic teeth to align properly even though the implants tilt
- Bone grafting becomes unnecessary for many patients who would otherwise require it
The All-on-4 protocol typically places two straight anterior implants and two angled posterior implants. Variations exist. All-on-6 protocols add two additional fixtures for enhanced support. Some cases call for three or four straight implants when bone volume proves generous.
| Protocol | Number of Implants | Typical Angulation | Indications |
|---|---|---|---|
| All-on-4 | 4 | Two straight, two angled at 30-45° | Standard edentulous arch; adequate anterior bone |
| All-on-6 | 6 | Four straight, two angled; or all straight | Enhanced support; parafunctional habits; opposing natural dentition |
| All-on-8 | 8 | All straight when bone allows | Maximum support; heavy bruxers; young patients |
| Zygomatic | 2-4 zygomatic + 0-4 standard | Zygomatic implants angled into cheekbone | Severe maxillary atrophy; no bone for conventional implants |
Important Note: The term “All-on-4” is a registered trademark of Nobel Biocare. Many clinics use alternative brand names for conceptually similar protocols. Focus on the clinical rationale, not the marketing terminology.
Materials Matter: What Your Implant Arch Is Made Of
The materials chosen for your implant arch affect aesthetics, durability, repairability, and cost. Surgeons and restorative dentists often have strong preferences based on their clinical experience. Understanding the options empowers you to participate meaningfully in treatment planning conversations.
Implant Materials: Titanium vs. Zirconia
Titanium Implants
Titanium and its alloys (primarily Ti-6Al-4V) dominate the implant market for excellent reasons. The material’s biocompatibility is superb. Osseointegration around titanium is well-documented over decades of clinical research. Titanium implants are strong, fracture-resistant, and available in countless designs from hundreds of manufacturers.
Titanium implants consist of two pieces typically—the fixture itself and a separate abutment. This two-piece design offers restorative flexibility. If the prosthetic arch requires modification years later, the abutment can be changed without disturbing the osseointegrated fixture.
Some patients express concern about metal sensitivity or dislike the idea of metal in their bodies. True titanium allergy is exceptionally rare. Trace metal ion release occurs but at levels far below clinically relevant thresholds.
Zirconia Implants
Zirconia implants offer an alternative for patients seeking metal-free solutions. Modern dental zirconia is yttria-stabilized tetragonal zirconia polycrystal (Y-TZP), a ceramic with remarkable strength and toughness. Zirconia implants are white, which provides aesthetic advantages in patients with thin gum tissue where titanium might show through as a gray shadow.
Zirconia currently comes primarily as one-piece implants, though two-piece designs are increasingly available. One-piece designs mean the implant and abutment are a single unit. This simplifies restorative protocols but reduces flexibility if future modification becomes necessary.
The long-term data on zirconia implants is shorter than that for titanium. While early results are encouraging, titanium remains the evidence-based standard. Some clinicians prefer zirconia for anterior single-tooth replacement. For full-arch restorations, titanium’s track record, design versatility, and connection strength favor its use in most cases.
Prosthetic Arch Materials: Acrylic, Composite, Zirconia, and Hybrid Designs
The prosthetic arch—the bridge containing your new teeth—can be fabricated from several materials or combinations. Each offers distinct advantages and limitations.
Acrylic with Titanium Bar Framework
The most common and cost-effective full-arch prosthesis combines a computer-milled titanium bar with heat-cured acrylic housing the denture teeth. The titanium bar provides structural rigidity. The acrylic offers aesthetic tooth arrangement and a gum-colored base.
Advantages include lower cost, repairability, and lighter weight. Should a tooth chip or fracture, a dental laboratory can typically repair an acrylic prosthesis without replacing the entire arch. The softer acrylic material also absorbs some occlusal forces, potentially protecting the underlying implants.
Limitations include greater wear over time. Acrylic teeth abrade more quickly than ceramic alternatives. The acrylic base can stain and will require polishing during maintenance visits. Expect to replace or significantly refurbish an acrylic arch after 5 to 10 years of service.
Monolithic Zirconia
Full-contour zirconia arches offer a premium option. These prostheses are milled entirely from a single block of highly esthetic zirconia, then sintered, stained, and glazed. The result is breathtakingly beautiful. Zirconia’s translucency and color depth mimic natural dentition remarkably well.
Advantages include extreme strength, outstanding wear resistance, and excellent biocompatibility. Zirconia arches resist chipping and fracturing far better than acrylic. They maintain their polish and appearance indefinitely with proper care.
Limitations include higher cost, heavier weight, and more difficulty repairing if damage does occur. Zirconia is also extremely hard, which means careful attention to occlusion is essential to protect opposing teeth or restorations from excessive wear. The material transmits occlusal forces more directly to the implants and bone, a consideration for patients with compromised bone quality.
Hybrid Designs: Zirconia-PMMA and PEKKTON
Newer materials attempt to combine the best properties of different material classes. Zirconia-reinforced PMMA (polymethyl methacrylate) offers improved aesthetics over traditional acrylic with better wear characteristics. PEKKTON, a high-performance polymer, provides strength with some flexibility and outstanding biocompatibility.
These materials represent the middle ground. They cost more than acrylic but less than monolithic zirconia. They offer aesthetic improvements over basic acrylic while maintaining some shock-absorbing qualities. Long-term data is limited, but early clinical reports are encouraging.
The Framework Options
Underneath the visible prosthetic teeth and gums sits a reinforcing framework. For acrylic prostheses, this framework is typically computer-milled titanium, custom-made for your specific implant positions and arch form. Some laboratories offer cobalt-chromium frameworks at lower cost, though the metal may provoke sensitivity in a small percentage of patients.
Zirconia arches may or may not include a separate framework. Monolithic designs are self-supporting. Some laboratories mill a thin titanium substructure and fuse zirconia to it, creating a hybrid with the aesthetics of zirconia and the implant-connection precision of titanium.
| Prosthetic Material | Average Lifespan | Repairability | Aesthetics | Relative Cost | Weight |
|---|---|---|---|---|---|
| Acrylic with Ti bar | 5-10 years | Excellent | Good | $$ | Light |
| Zirconia-reinforced PMMA | 7-12 years | Moderate | Very good | $$$ | Moderate |
| PEKKTON hybrid | 8-15 years | Moderate | Very good | $$$ | Light |
| Monolithic Zirconia | 10-20+ years | Difficult | Excellent | $$$$ | Heavy |
The Candidacy Question: Are You Eligible for a Dental Implant Arch?
Not every patient with missing teeth qualifies immediately for a dental implant arch. Candidacy depends on medical, anatomical, and behavioral factors. An honest assessment saves you from disappointment and complications.
Medical Considerations That Influence Candidacy
Uncontrolled Systemic Disease
Diabetes with hemoglobin A1c persistently above 8.0% impairs wound healing and osseointegration. Immunocompromised patients face elevated infection risk. Active cancer treatment, particularly radiation to the head and neck region, significantly complicates implant surgery.
These conditions do not necessarily disqualify you permanently. Getting your diabetes under better control may open the door to treatment. Completing cancer therapy and allowing a healing interval may restore eligibility. Your surgeon will coordinate with your physician to optimize your medical status before proceeding.
Medication Profiles
Intravenous bisphosphonates and certain other antiresorptive medications, used primarily in cancer patients, create substantial risk for medication-related osteonecrosis of the jaw (MRONJ). Oral bisphosphonates for osteoporosis carry lower but non-zero risk. Your surgeon must know every medication you take, including supplements.
Anticoagulant and antiplatelet medications require careful perioperative management. Your surgeon will coordinate with your prescribing physician regarding temporary cessation or bridging protocols when appropriate.
Smoking and Tobacco Use
Smoking dramatically impairs healing and increases implant failure rates. Most implant surgeons strongly recommend smoking cessation at least two weeks before and eight weeks after surgery. Some will not treat active smokers at all for full-arch cases given the stakes and investment involved.
This is not moral judgment. It is clinical reality. The vasoconstrictive effects of nicotine starve healing tissues of oxygen. The heat and chemicals in tobacco smoke irritate surgical sites. The failure rate difference between smokers and non-smokers is statistically significant and clinically meaningful.
Anatomical Requirements
Bone Volume and Density
Implants require adequate bone for primary stability at placement and long-term osseointegration. Years after tooth loss, the alveolar ridge resorbs significantly. In the posterior maxilla, the maxillary sinus expands downward, leaving minimal bone height beneath it. In the posterior mandible, the inferior alveolar nerve limits implant length.
Cone beam computed tomography (CBCT) scans provide three-dimensional assessment of your available bone. Surgeons evaluate height, width, and density at each planned implant site. They identify critical anatomical structures and plan implant positions that avoid them.
When bone volume proves insufficient, several strategies exist:
- Bone grafting adds volume from another site or a donor source
- Angled implant placement bypasses deficient areas
- Zygomatic implants anchor in the cheekbone when maxillary bone is absent
- Short or reduced-diameter implants work in narrow ridges
- Ridge splitting or expansion creates space for implants in thin bone
Soft Tissue Health
Healthy gums are not just aesthetically important. The peri-implant soft tissue seal—the biological barrier where gum meets implant or abutment—protects underlying bone from bacterial invasion. Active periodontal disease, mucosal lesions, or inadequate attached gingiva require pretreatment.
Some patients need soft tissue grafting to establish an adequate zone of keratinized tissue around implants. Others need periodontal therapy to resolve active infections before implant placement. Your surgeon’s examination considers these factors carefully.
The Psychological Readiness Factor
Full-arch implant treatment represents a significant commitment. The process takes months. There will be temporary prostheses, dietary restrictions, and healing phases. You will spend considerable money. You must maintain meticulous oral hygiene indefinitely.
Honest self-assessment matters. Are you prepared for the surgical component? Can you follow post-operative instructions carefully? Will you attend maintenance appointments? Can you adjust to a fixed restoration that feels different from natural teeth or dentures?
Patients who approach treatment with realistic expectations and strong commitment enjoy the best outcomes. Those seeking a quick fix or expecting perfection without effort may find the journey more challenging.
The Treatment Journey: From Consultation to Final Restoration
Understanding the sequence of appointments demystifies the process and reduces anxiety. The journey follows a logical progression, though specific protocols vary between practitioners and cases.
Phase One: Comprehensive Assessment and Planning
Your first visit consumes significant time—often two hours or more. The prosthodontist or restorative dentist leads this evaluation, often working alongside the surgeon from the beginning. This collaborative approach improves outcomes dramatically compared to dentist-surgeon teams that communicate only through referral forms.
Records Gathering
The team acquires a complete set of diagnostic records. Photographs document your current facial and dental appearance. Digital or conventional impressions capture your existing dentition and ridge anatomy. A CBCT scan provides the three-dimensional bone imaging essential for implant planning. Some practices also capture jaw motion recordings and facial scans for advanced virtual planning.
The Clinical Examination
The dentist examines your oral tissues, remaining teeth, existing restorations, and ridge morphology. They assess your smile line, lip support, and facial proportions. They discuss your goals and expectations. They identify any pathology requiring treatment before implant surgery, such as decay, infection, or soft tissue lesions.
Multidisciplinary Treatment Planning
Complex full-arch cases often benefit from input from multiple specialists. A prosthodontist may lead the restorative design. An oral surgeon or periodontist plans the surgical placement. A dental laboratory technician may participate in virtual design sessions. Some practices bring all parties together for treatment planning conferences.
Virtual Surgical Planning
Modern implant dentistry employs sophisticated software to plan implant positions virtually before any scalpel touches tissue. The planning team merges your CBCT data with digital scans of your teeth and soft tissues. They select virtual implants, position them in ideal locations, and design the planned prosthesis.
From this virtual plan, the team can fabricate surgical guides that direct implant placement with exceptional accuracy. These guides, 3D-printed in a laboratory, fit over your ridge or teeth and feature metal sleeves that guide the surgeon’s drills. Guided surgery improves precision, reduces surgical time, and often allows less invasive flap designs.
Phase Two: Preparatory Procedures
Some patients require interventions before implant placement. The treatment plan identifies these needs during the assessment phase.
Tooth Extractions
If failing teeth remain in the arch, the surgeon removes them. In immediate-loading protocols, extractions and implant placement often occur in the same surgical appointment. In delayed protocols, extractions happen first, followed by a healing interval before implant surgery.
Extraction technique matters. The surgeon aims to preserve as much bone as possible, minimizing trauma to the socket walls. They thoroughly debride the sockets of granulation tissue and infection. Some sockets receive bone graft material to preserve ridge dimensions for subsequent implant placement.
Bone Grafting
When existing bone volume cannot support implants, grafting adds the necessary substrate. Autogenous grafts, harvested from your own body (typically mandibular ramus, chin, or iliac crest), offer the best regenerative potential. Allografts from human tissue banks, xenografts from bovine sources, and alloplastic synthetic materials provide alternatives without a donor site.
Major bone grafting procedures require their own healing period—often four to six months—before implant placement becomes possible. This extends the overall timeline but creates the foundation necessary for long-term success.
Sinus Augmentation
In the posterior maxilla, insufficient bone height beneath the maxillary sinus often necessitates a sinus lift procedure. The surgeon accesses the sinus through a small window in the lateral maxillary wall or through the implant osteotomy itself. They carefully elevate the sinus membrane and pack bone graft material into the created space. Over several months, this graft matures into implant-ready bone.
Phase Three: Implant Placement Surgery
Surgery day arrives. Your specific experience depends on the protocol selected and your personal preferences for sedation.
Anesthesia and Sedation Options
Most full-arch implant surgeries proceed under intravenous sedation or general anesthesia, particularly for complex cases. Conscious sedation allows you to breathe independently but keeps you deeply relaxed with minimal memory of the procedure. General anesthesia provides complete unconsciousness. Some patients elect local anesthesia only, though lengthier procedures test even stoic patients.
The Surgical Procedure
The surgeon prepares the surgical site, typically raising a full-thickness flap to visualize the bone directly. When using a surgical guide, flap reflection may be more limited or eliminated entirely with flapless techniques.
The surgeon then creates osteotomies—precise holes in the bone—using a sequence of progressively larger drills. Copious irrigation prevents overheating that could damage bone cells. Each implant is placed to the planned depth and torque. The surgeon checks primary stability; adequate resistance to rotation indicates the implant is ready for loading, either immediately or after a healing period.
Multi-unit abutments are often connected to the implants at this stage. They extend through the gum tissue and will eventually receive the prosthetic arch. The surgeon may take an impression or digital scan to facilitate immediate prosthesis fabrication.
Closure and Immediate Post-Operative Care
The surgeon sutures the gum tissue around the implants and abutments. You move to a recovery area where staff monitor your vital signs as sedation wears off. You receive detailed post-operative instructions, prescriptions for pain management and antibiotics when indicated, and a follow-up schedule.
Phase Four: The Provisional Restoration
The period between implant placement and delivery of the final prosthesis requires a temporary solution. Options depend on the treatment protocol.
Immediate Loading Protocols
In selected cases, patients leave surgery with fixed temporary teeth the same day or within 48 hours. The surgeon and restorative team fabricate a provisional prosthesis—usually an acrylic arch reinforced with a metal framework—that screws onto the implants. This “conversion prosthesis” provides function and aesthetics during the osseointegration period.
Immediate loading requires excellent primary stability of all implants and a splinted, rigid provisional restoration. The prosthesis minimizes micromovement that could disrupt osseointegration. Patients follow a strict soft-food diet during the initial healing weeks.
Not all patients qualify for immediate loading. Risk factors include poor bone quality, inadequate primary stability, extensive grafting, and certain medical conditions. Your surgeon determines suitability based on objective criteria measured at the time of implant placement.
Delayed Loading Protocols
When conditions do not favor immediate loading, patients wear a conventional removable denture or a healing prosthesis during osseointegration. The surgeon modifies an existing denture or fabricates a new one to avoid pressure on the healing implants. Patients remove this prosthesis for sleeping and cleaning.
This approach sacrifices immediate fixed function for what some surgeons consider a more conservative, lower-risk healing environment. The implants osseointegrate undisturbed for three to six months before prosthetic loading begins.
Phase Five: Final Prosthesis Fabrication
After osseointegration is confirmed—typically three to six months after placement—the restorative phase culminates in delivery of the definitive prosthesis.
Implant-Level Impressions
The restorative dentist takes precise impressions of the implant positions. Traditional techniques use impression copings and polyvinyl siloxane material. Digital workflows employ intraoral scanners and scan bodies attached to the implants. Both methods capture the three-dimensional spatial relationship of the implants to each other and to the opposing arch.
Jaw Relation Records
The dentist records how your jaws relate to each other—your bite registration. This captures vertical dimension (facial height), centric relation, and occlusal plane orientation. Wax rims or trial bases help establish aesthetic parameters including tooth position, lip support, and smile line.
Trial Insertion
For most cases, the laboratory provides a wax or acrylic trial set-up. You see the proposed tooth arrangement in your mouth before final fabrication. This crucial step allows you and your dentist to evaluate aesthetics, phonetics, and function. Adjustments requested at this stage are straightforward to implement.
Final Delivery
The completed prosthesis arrives from the laboratory. The dentist seats it, verifies passive fit, adjusts occlusion, and evaluates aesthetics. You approve the result. The dentist tightens the retaining screws to the manufacturer-specified torque and seals the access holes with composite or cotton and composite.
You now have your permanent fixed implant arch.
Living with an Implant Arch: Daily Reality and Long-Term Care
The transition to living with an implant arch is mostly joyful but requires some adaptation. Understanding the maintenance commitment protects your significant investment.
The Adaptation Period
First Days and Weeks
Your new arch feels foreign initially. The prosthesis occupies space your brain previously registered as empty. Your tongue explores the new contours. Speech feels slightly different, particularly for “s” and “th” sounds. This passes quickly—usually within a week or two—as your oral musculature adapts.
For immediate-loading cases, dietary restrictions are strict during early healing. Soft foods only for the first several weeks. Gradual introduction of firmer textures as comfort allows and your surgeon permits. For conventional loading, the conversion to fixed teeth feels revelatory. Patients report emotional moments when they first see themselves in the mirror.
Speech Adaptation
Reading aloud to yourself accelerates speech adaptation. Practice words heavy in sibilants and fricatives. Record yourself speaking and listen critically. Most patients report normal speech within two weeks. A small minority require minor prosthetic adjustments to improve phonetic clarity—slightly narrowing the palatal contours of an upper prosthesis often resolves lingering lisp issues.
Sensory Differences
Fixed implant arches lack the periodontal ligament proprioception of natural teeth. You do not feel the same fine tactile feedback when biting. Your brain compensates using feedback from the muscles of mastication, the temporomandibular joint, and the opposing arch. Adaptation occurs over weeks to months.
You also lack thermal sensation through the prosthetic teeth. Hot coffee does not feel hot against the teeth themselves, though you feel temperature on your tongue, palate, and surrounding soft tissues. This poses minor burn risks initially; test hot foods and beverages carefully until you adjust.
Hygiene Protocols for Long-Term Success
Peri-implant diseases—mucositis and peri-implantitis—represent the greatest long-term threat to implant survival. Meticulous hygiene prevents these inflammatory conditions from compromising your investment.
Daily Home Care
You need specific tools beyond a standard toothbrush. Interdental brushes access the spaces between implants and under the prosthetic arch. Water flossers with non-metal tips flush debris from around abutments. Floss threaders or superfloss clean under the prosthesis where it contacts the gum tissue. Your dentist or hygienist demonstrates these techniques during maintenance visits.
Twice-daily brushing with a soft toothbrush suffices for the prosthetic teeth and gums. Non-abrasive toothpaste prevents scratching the prosthesis surface. Some patients benefit from antimicrobial mouth rinses, particularly those with a history of periodontal disease.
Professional Maintenance
You will visit your dentist or hygienist for professional maintenance at intervals determined by your individual risk profile—typically every three to six months. These visits include thorough cleaning around implants with specialized plastic or titanium instruments that do not scratch abutment surfaces.
The clinician removes the prosthesis periodically for inspection and deep cleaning. They examine the implant-abutment connections, assess soft tissue health, and polish the prosthesis. Removal frequency varies among practitioners; some remove the prosthesis annually, others every two to three years unless problems arise.
Longevity and Replacement Expectations
Dental implant arches do not last forever, though the implants themselves can last decades or a lifetime with proper care. The prosthetic components have finite lifespans.
Implant Survival Rates
Systematic reviews report implant survival rates exceeding 95% over ten years for full-arch rehabilitations. Factors that reduce survival include smoking, poor oral hygiene, uncontrolled diabetes, and parafunctional habits like bruxism. Regular maintenance and early intervention when problems arise maximize implant longevity.
Prosthesis Replacement Intervals
The prosthetic arch requires replacement or major refurbishment on a predictable schedule:
- Acrylic-titanium hybrid prostheses: 5-10 years typically
- Zirconia-reinforced PMMA: 7-12 years
- Monolithic zirconia: 10-20+ years
Replacement triggers include excessive wear, fracture, deteriorating aesthetics, loosening of denture teeth, or changes in fit due to ongoing ridge resorption. Budgeting for eventual replacement represents a prudent financial planning step.
Financial Realities: Understanding the Investment
Full-arch implant treatment represents a significant financial commitment. Transparency about costs, insurance considerations, and financing options helps you make informed decisions.
Cost Components and Ranges
The total fee for a single-arch implant restoration encompasses multiple elements. Understanding these components helps you compare treatment plans from different providers.
Surgical Fees
The surgeon’s fee covers implant placement, any necessary extractions, bone grafting, and related surgical procedures. Fees vary by surgeon specialty, experience, and geographic location. Oral and maxillofacial surgeons and periodontists typically charge within similar ranges, though individual variation exists.
Restorative Fees
The restorative dentist’s fee covers treatment planning, provisional restorations, final impressions, fabrication coordination, delivery, and follow-up adjustments. The complexity and material selection significantly influence this component.
Laboratory Fees
Dental laboratories charge for fabricating the prosthesis. This fee reflects the materials used, the technician’s skill, and the technological sophistication involved. A milled titanium framework with acrylic prosthesis costs less than a fully monolithic zirconia restoration.
Anesthesia and Facility Fees
When treatment occurs under intravenous sedation or general anesthesia, associated fees apply. Procedures performed in hospital settings or ambulatory surgery centers incur facility charges beyond the surgeon’s professional fee.
| Cost Component | Lower Range | Typical Range | Higher Range |
|---|---|---|---|
| Surgical placement (per arch) | $8,000 | $12,000 – $18,000 | $25,000+ |
| Restorative phase | $5,000 | $8,000 – $15,000 | $20,000+ |
| Laboratory (prosthesis) | $3,000 | $5,000 – $10,000 | $15,000+ |
| Provisional restoration | $1,500 | $2,500 – $5,000 | $7,500+ |
| Anesthesia/facility | $500 | $1,500 – $3,500 | $6,000+ |
| Pre-treatment procedures (grafting, extractions) | $1,000 | $3,000 – $8,000 | $15,000+ |
| Total Estimated Cost per Arch | $19,000 | $32,000 – $60,000 | $90,000+ |
Important Note: These figures reflect fee-for-service private practice pricing in the United States in 2026. Dental school clinics, residency programs, and some corporate practices offer lower fees. International dental tourism destinations may advertise prices substantially lower, though quality, follow-up care, and liability recourse vary enormously. Research carefully before traveling for treatment.
Insurance Considerations
Medical and dental insurance benefits for implant treatment vary widely. Most dental insurance plans classify implants as a major service with 50% coverage up to an annual maximum, typically $1,500 to $3,000. This contributes modestly to a significant treatment cost.
Some medical insurance policies cover portions of implant treatment when tooth loss results from trauma, congenital conditions, or disease requiring medical management. Coverage determinations depend on your specific plan language, the documentation your providers submit, and often, persistent advocacy on your behalf.
Flexible spending accounts (FSAs) and health savings accounts (HSAs) allow you to pay for implant treatment with pre-tax dollars when the treatment qualifies as a medical expense. Consult your tax advisor regarding eligibility.
Financing Options
Most implant practices offer or facilitate financing. Third-party healthcare lenders like CareCredit, LendingClub, and Proceed Finance provide dedicated medical loans with promotional interest-free periods, often 6 to 24 months. Extended-term financing at competitive interest rates extends repayment over several years.
Some practices offer in-house payment plans structured as the treatment progresses. Others provide discounts for payment in full at treatment initiation. Discuss financial arrangements openly with the treatment coordinator. Reputable practices welcome these conversations and present options transparently.
Many patients combine multiple funding sources—insurance reimbursement, HSA funds, a healthcare credit card for the remainder, and perhaps family assistance. A clear financial plan reduces the anxiety that might otherwise shadow your treatment experience.
Risks and Complications: Honest Disclosure
Every surgical and restorative procedure carries risk. Understanding potential complications empowers you to recognize problems early and seek appropriate intervention. Honest discussion of risks does not imply that complications are likely—most implant arches heal uneventfully and serve patients well for many years—but pretending complications never occur serves no one.
Surgical Complications
Intraoperative Events
During implant placement, the surgeon navigates near critical anatomical structures. Damage to the inferior alveolar nerve in the mandible causes temporary or, rarely, permanent numbness of the lower lip and chin. Perforation of the maxillary sinus membrane typically heals uneventfully but may require additional management. Excessive bleeding is uncommon in healthy patients but requires prompt control.
Surgeons mitigate these risks through careful preoperative imaging, surgical guides, and experience. Informed consent includes discussion of site-specific anatomical risks.
Postoperative Issues
Swelling, bruising, and discomfort peak two to three days after surgery and then subside. Infection occurs in a small percentage of cases despite sterile technique and prophylactic antibiotics. Wound dehiscence—opening of the incision—occasionally exposes implant cover screws or bone graft material. Most such complications resolve with conservative management. Frank implant infection in the early postoperative period is rare but serious.
Restorative Complications
Prosthetic Fracture
The prosthesis can fracture under excessive load. Acrylic prostheses fracture more readily than zirconia. Fracture risk increases over time as materials fatigue. Most fractures occur in patients with heavy bite forces, parafunctional habits, or opposing implant-supported restorations that generate high occlusal forces. Repair or replacement addresses the issue, though the underlying cause should be identified and managed.
Screw Loosening
The retaining screws that secure the prosthesis to the implants occasionally loosen. You may notice slight movement, clicking, or a change in the prosthesis feel. Your dentist can retighten or replace loose screws. Systematic screw loosening suggests occlusal overload, framework misfit, or parafunction requiring attention.
Aesthetic Compromises
Gum recession around implants may expose abutment metal over time. Acrylic prosthesis staining or wear affects appearance gradually. Changes in facial anatomy with aging may alter the relationship between the prosthesis and your lips. These issues are typically addressable through prosthetic modification or replacement.
Long-Term Biological Complications
Peri-Implant Mucositis
Inflammation of the soft tissue surrounding implants, analogous to gingivitis around natural teeth, is common. Bleeding on probing, redness, and swelling characterize this condition. Mucositis is reversible with improved hygiene and professional debridement. Left untreated, it may progress to peri-implantitis.
Peri-Implantitis
This destructive inflammatory condition involves both soft tissue inflammation and progressive bone loss around implants. Prevalence varies in the literature, but some studies suggest 10-20% of implants develop peri-implantitis over ten years. Risk factors include poor oral hygiene, smoking, history of periodontitis, diabetes, and irregular maintenance care.
Treatment ranges from nonsurgical debridement for early lesions to surgical access, decontamination, and regenerative procedures for advanced defects. Severe peri-implantitis may cause implant loss. Prevention through meticulous hygiene and regular professional maintenance remains the cornerstone of management.
The Opposing Arch Dilemma: What Faces the Implant Arch?
The teeth or restoration opposing your implant arch significantly affect long-term outcomes. This consideration sometimes receives insufficient attention during treatment planning.
Natural Teeth Opposing an Implant Arch
Natural teeth exert lower bite forces than implant-supported prostheses typically. When a zirconia or acrylic implant arch opposes natural teeth, careful attention to occlusal design prevents excessive wear of the natural dentition. The natural teeth should contact evenly with the prosthesis during function.
Some patients have natural teeth in good condition on one arch and require implant restoration on the other. This asymmetrical situation functions well when properly managed. The natural teeth require continued preventive care. Your dentist monitors wear patterns at maintenance visits.
Conventional Dentures Opposing an Implant Arch
A common scenario involves an implant-retained lower arch opposing a conventional maxillary denture. The stability and force generation of the implant arch may accelerate wear on the opposing denture teeth and contribute to denture base instability. Many patients proceed with converting the conventional denture to an implant-supported restoration when budget allows.
In the interim, the dentist can place harder denture teeth in the conventional prosthesis to resist wear. Regular relines maintain fit as the edentulous ridge continues to resorb under the removable prosthesis.
Two Opposing Implant Arches
Patients who restore both arches with implant-supported prostheses report the highest satisfaction. Both arches remain fixed, stable, and functional. Careful attention to occlusal scheme becomes important. The dentist must design the occlusion to distribute forces evenly, avoid interferences during jaw movements, and protect both prostheses and supporting implants.
As these patients generate the highest bite forces of any restoration combination, robust prosthetic design is essential. Many clinicians recommend zirconia or high-performance polymer prostheses for patients opposing another implant arch.
Dental Tourism for Implant Arches: A Balanced Perspective
International treatment for full-arch implant rehabilitation attracts patients seeking lower costs. Several destinations have developed substantial dental tourism infrastructure. An honest assessment includes both potential benefits and real risks.
Potential Advantages
Cost represents the primary motivation. Clinics in Mexico, Costa Rica, Hungary, Thailand, and other destinations may advertise full-arch treatments at 40-60% less than U.S. fees. These savings reflect lower labor costs, reduced regulatory burden, and different economic conditions.
Some international clinics boast impressive facilities, Western-trained clinicians, and sophisticated technology. Patients who research carefully and select reputable providers may receive excellent care at meaningful savings.
Significant Risks and Considerations
Continuity of Care
Postoperative complications, prosthetic adjustments, and long-term maintenance require access to a treating clinician. Patients who travel for treatment often lack this continuity. Finding a local provider willing to manage complications from another clinician’s work presents challenges. Emergency issues may require urgent travel or go unmanaged.
Standard of Care Variation
Regulatory standards, infection control protocols, and material authenticity verification vary internationally. Counterfeit implant components exist in some markets. Sterilization standards may not meet U.S. expectations. Detailed due diligence is essential but difficult to accomplish from abroad.
Liability and Recourse
Legal recourse for substandard treatment across international borders ranges from difficult to impossible. U.S. malpractice insurance and legal protections do not extend overseas. Patients accept these limitations, often without fully appreciating the implications.
Travel Logistics
Multiple visits are typically required, even for “one-visit” protocols heavily marketed to international patients. Complications may necessitate additional unplanned travel. Recovery while traveling—potentially alone in a hotel room—differs significantly from recovering at home with established support systems.
The Hidden Cost Calculation
When accounting for travel expenses, accommodations, time away from work, and the potential costs of managing complications domestically, the net savings may prove less substantial than advertised fees suggest. A realistic total-cost analysis informs smarter decisions.
Suggestion: If considering dental tourism, request the treating clinician’s curriculum vitae, facility photographs and accreditation documentation, material certificates of authenticity, and a detailed treatment plan with all fees. Speak directly with former patients who received similar treatment. Visit the facility in advance if possible. Research the local dental regulatory body and any disciplinary records.
Questions to Ask Your Provider Before Treatment
An informed patient is the best partner in treatment. The consultation represents your opportunity to evaluate the provider, the plan, and your comfort level. Bring these questions to your appointment.
Questions About the Provider and Team
“Who performs the surgery, and who restores the prosthesis?”
Some practices have an in-house surgeon and restorative dentist who collaborate closely. Others refer between separate offices. Both models can work well. Ensure you understand who handles each phase and how they communicate.
“How many full-arch cases have you completed?”
Volume and experience matter. Surgeons who perform full-arch rehabilitation regularly manage complications efficiently and approach planning with seasoned judgment. Ask about specific numbers rather than accepting general assurances.
“May I see cases similar to mine with before and after photographs?”
Reviewing documented outcomes helps you assess aesthetic sensibilities and consistency. Look for cases that match your situation—fully edentulous, failing dentition, similar bone volume.
Questions About the Specific Treatment Plan
“Why did you select this number of implants for my case?”
The answer reveals the clinical reasoning behind the plan. Four implants? Six? Eight? Zygomatic? Each choice reflects assessment of your anatomy, bone quality, opposing dentition, and risk factors. The clinician should articulate this rationale clearly.
“What materials do you recommend for my prosthesis, and why?”
The recommendation should reference your specific circumstances—functional demands, aesthetic priorities, budget, opposing dentition, parafunctional habits. Generic recommendations suggest generic thinking.
“What provisional restoration will I wear during healing?”
Understand whether you will receive an immediate fixed prosthesis, a modified denture, or no prosthesis at all during osseointegration. This significantly affects your experience during the months of treatment.
Questions About Risks and Long-Term Care
“What specific complications concern you most in my case?”
An honest clinician identifies patient-specific risk factors and discusses mitigation strategies. Beware of anyone who dismisses risk entirely.
“What maintenance schedule do you recommend, and what does it cost?”
Long-term maintenance represents an ongoing commitment of time and money. Understand what you are signing up for beyond the initial treatment.
“What is your protocol when a complication arises—on a Tuesday afternoon or a Saturday night?”
Availability for urgent concerns matters. A practice without after-hours coverage leaves you navigating emergencies alone.
Innovations on the Horizon
Implant dentistry continues advancing. Several emerging technologies are reshaping full-arch rehabilitation and may influence your treatment decisions.
Digital Workflow Maturation
Fully digital workflows—from intraoral scanning to virtual implant planning to computer-aided manufacturing—continue improving in accuracy and accessibility. Same-day restoration fabrication using in-office milling or 3D printing is moving from novelty to standard practice in advanced clinics.
Artificial intelligence assists in implant planning algorithms, identifying optimal implant positions based on bone density, anatomical constraints, and prosthetic requirements. These tools augment rather than replace clinician judgment, but they add objective data to the planning process.
New Materials and Surface Technologies
Implant surface modifications continue to evolve. Hydrophilic surfaces accelerate osseointegration. Nanostructured topographies may enhance bone response. Antibacterial coatings or eluting surfaces aim to reduce peri-implant disease risk.
Prosthetic materials are progressing rapidly. High-performance polymers like PEKK and advanced composites offer new combinations of strength, aesthetics, and repairability. Gradient zirconia with varying translucency replicates natural tooth appearance more convincingly than homogeneous blocks.
Minimally Invasive Protocols
Flapless surgery guided by 3D-printed surgical templates reduces postoperative morbidity. Piezoelectric surgical instruments cut bone with minimal soft tissue trauma. Smaller-diameter implants and shorter implant designs expand candidacy without extensive grafting. The trend favors less invasive approaches when clinically appropriate.
Conclusion
A dental implant arch is a permanent, fixed row of prosthetic teeth secured to surgically placed dental implants, designed to replace an entire upper or lower set of missing teeth and restore near-natural function, aesthetics, and facial support. This comprehensive guide details the entire journey—from understanding the biological foundation of osseointegration and the biomechanics of load distribution to navigating the surgical phases, prosthetic material choices, financial planning, and lifelong maintenance commitments. Ultimately, the treatment delivers transformative quality-of-life improvements for patients suffering from extensive tooth loss, though it requires careful candidacy evaluation, realistic expectations, and unwavering dedication to daily hygiene and professional follow-ups.
Frequently Asked Questions
Can I sleep with my implant arch in place?
Yes. A fixed implant arch is designed to remain in your mouth 24 hours a day. Unlike traditional dentures, you do not remove it for sleeping. Only your dentist removes the prosthesis during periodic maintenance visits for inspection and deep cleaning.
How painful is the implant surgery?
Most patients report less discomfort than anticipated. The surgical sites are typically sore for three to five days, manageable with prescribed or over-the-counter analgesics. Intravenous sedation during surgery means you recall little of the procedure itself. Soft tissue healing progresses rapidly, and many patients transition to non-narcotic pain control within 48 hours.
Will people know I have an implant arch?
Modern implant arches are highly aesthetic. When designed and fabricated skillfully, they look natural to casual observers and even to close family members. The absence of a visible palatal plate—present in upper dentures—contributes significantly to the natural feel. Speech adapts quickly. Within weeks, most patients report that others perceive no difference from natural teeth.
What happens if one implant fails?
Implant failure is uncommon but not unknown. If an implant fails before the final prosthesis is fabricated, the surgeon can often place another implant, sometimes in an alternative position, without disrupting the overall plan. If an implant supporting a final prosthesis fails, the remaining implants may continue to support the arch depending on the number and distribution of fixtures. In some cases, the prosthesis requires modification or replacement, and a new implant is placed. This underscores the value of placing adequate implants from the outset.
How do I choose between four, six, or eight implants?
The decision balances anatomical constraints, risk tolerance, and budget. Four implants using angled posterior placement may suffice for many patients with adequate bone. Six or eight implants provide redundancy—if one implant develops problems, the others can often maintain function without immediate surgical intervention. Patients with opposing implant arches, heavy bite forces, or a desire for maximum long-term stability often benefit from more implants. Your surgeon’s CBCT analysis and clinical experience guide this recommendation.
Additional Resource
For further reading on implant dentistry standards and patient education, visit the American College of Prosthodontists at www.prosthodontics.org. Their patient resources section offers additional information on tooth replacement options and finding qualified specialists.
Disclaimer: This article provides educational information only and does not constitute medical or dental advice. Every patient’s situation is unique. Diagnosis and treatment planning require comprehensive examination by a qualified dental professional. Discuss all treatment options, risks, and expected outcomes with your dental provider. Never delay seeking professional care based on information read online.



