What is Dental Bone Grafting? A Complete Guide for Patients
If you have recently visited a dentist and heard the words “bone graft,” you might have felt a little knot form in your stomach. It sounds complex, invasive, and perhaps a bit frightening. Let me reassure you right away: dental bone grafting is one of the most common, safe, and successful procedures performed in dentistry today.
In simple terms, a dental bone graft is a surgical procedure that replaces missing bone in your jaw. The goal is to create a solid foundation so you can place dental implants or simply restore the natural shape of your face and gums.
Think of your jawbone as the soil in a garden. If the soil erodes, you cannot plant a tree. A bone graft is the act of adding fresh, healthy soil so that tree (the dental implant) can grow strong and stable.
In this guide, we will walk through every detail you need to know. We will cover why you might need a graft, the different types of materials used, what happens during surgery, recovery tips, costs, and alternatives. By the end, you will feel informed, confident, and ready to talk to your dentist.
Understanding the Basics: Why Does the Jawbone Disappear?
Before we dive into the graft itself, it helps to understand why the bone in your mouth vanishes in the first place. The human body is incredibly efficient. If it detects that a part is no longer needed, it reabsorbs the tissue to use the minerals elsewhere.
Here are the primary reasons for jawbone loss:
- Tooth Extraction: When a tooth is removed, the roots are gone. The jawbone no longer receives stimulation from chewing. Over time, the bone shrinks.
- Periodontal Disease (Gum Disease): Severe gum disease destroys the soft tissue and the bone that holds your teeth in place.
- Trauma or Injury: An accident that knocks out teeth can also fracture or damage the bone.
- Empty Spaces: If you have had missing teeth for years, the bone in that area naturally deteriorates.
- Infection or Cysts: Large infections at the root of a tooth can dissolve the surrounding bone.
Important Note for Readers: Bone loss does not hurt. You likely will not feel your jaw shrinking. This is why regular x-rays are vital. Your dentist can spot bone loss long before it becomes a major problem.
Defining the Procedure: What is Dental Bone Grafting?
Let us answer the core question directly. What is dental bone grafting?
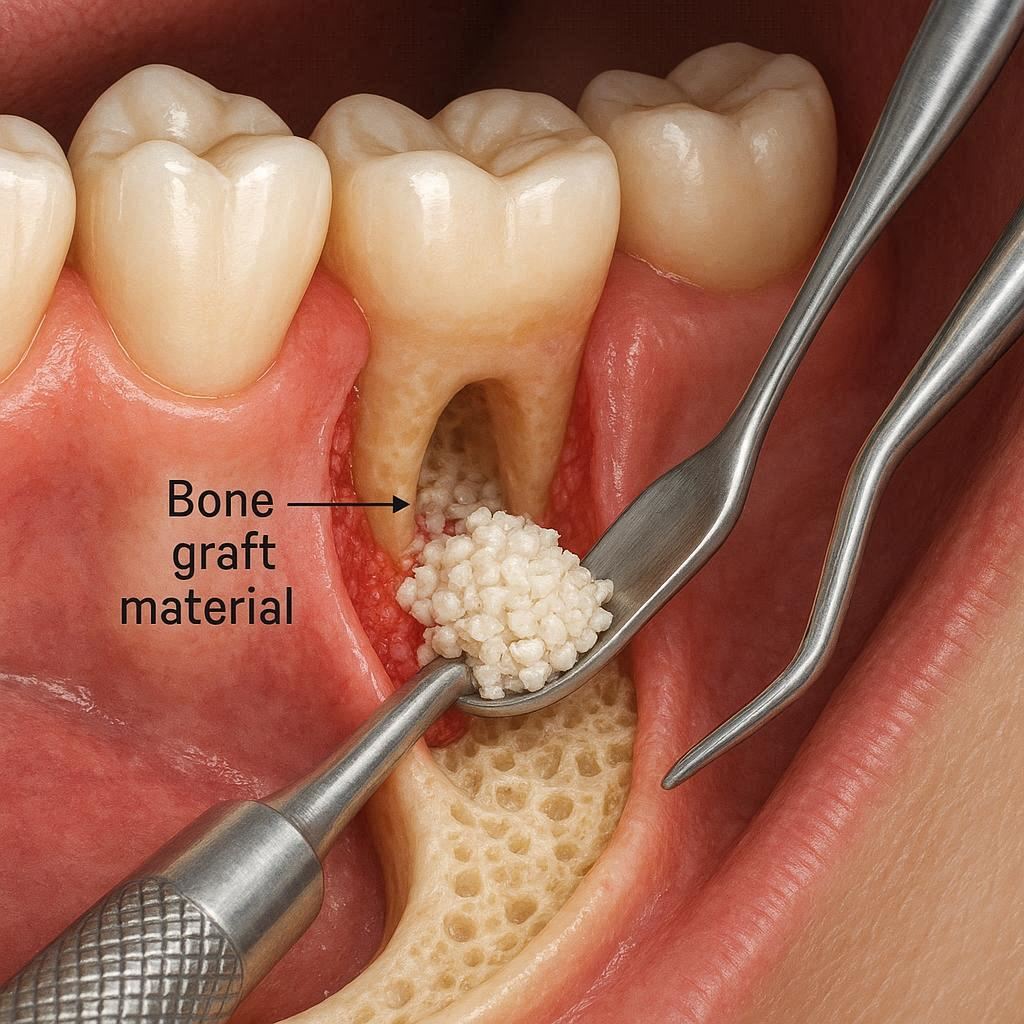
It is a regenerative procedure. Your dentist or oral surgeon takes bone material—either from your own body, a donor, an animal, or a synthetic source—and places it into an area of your jaw that has lost bone mass.
Over several months, this graft material acts like a scaffold. Your body’s natural healing cells migrate into that scaffold. Gradually, they break down the graft particles and replace them with your own, living, natural bone.
The procedure does not “instantly” give you hard bone. Instead, it encourages your body to rebuild its own bone.
The Role of Osseointegration
There is a fancy word you will hear often: osseointegration (ah-see-oh-in-teh-gray-shun). This is the process where living bone fuses directly to a surface—either a graft or an implant. A successful bone graft relies entirely on good osseointegration. If the graft integrates well, you are ready for the next step.
Signs You Might Need a Bone Graft (Without Knowing It)
Many patients walk into a dental clinic expecting a simple implant, only to be told they need a bone graft first. Here are the common signs and situations that lead to this recommendation:
- You have been missing a tooth for over a year. The bone shrinks most rapidly in the first six months after an extraction.
- Your dentures wobble or fall out. This often indicates the ridge of bone has flattened.
- You feel a dent in your gum. Run your tongue over an area where a tooth is missing. If it feels like a dip or trench, bone loss has occurred.
- You had severe gum disease. Even if you kept the teeth, the bone levels might be too low for implants.
- You are a smoker. Smoking accelerates bone loss significantly.
“I wish patients knew that a bone graft is not a failure. It is simply a detour on the road to a perfect smile. Almost half of my implant patients need some form of grafting.” — Dr. Elena Vasquez, Prosthodontist.
The Different Types of Dental Bone Grafts
Not all bone grafts are the same. Depending on your specific needs, budget, and medical history, your dentist will recommend one of four main types. Below is a table to help you compare them side-by-side.
| Type of Graft | Material Source | Pros | Cons | Typical Cost Level |
|---|---|---|---|---|
| Autograft | Your own body (usually jaw, chin, or hip) | Gold standard; contains living cells; fastest healing | Requires a second surgical site; more pain; longer surgery | High |
| Allograft | Human cadaver donor (sterilized) | No second surgery; safe; widely available | Slower integration than autograft; no living cells | Medium |
| Xenograft | Animal (usually cow or pig bone) | Very safe; excellent scaffolding; long history of use | Slowest to turn into human bone; purely mineral | Low to Medium |
| Alloplast | Synthetic (lab-made calcium or glass ceramics) | No risk of disease; unlimited supply; predictable | Fragile in some cases; lacks natural proteins | Low |
A Deeper Look at Each Graft Type
Autografts: The “gold standard.” Your surgeon takes a small piece of bone from your chin, your wisdom tooth area, or rarely your hip. Because it is your own tissue, there is zero risk of rejection. However, many patients dislike the idea of two wounds: one in their mouth and one in their hip or jaw.
Allografts: This is the most common type used today. The donor bone is rigorously processed, cleaned, and sterilized to remove all cells and water. Only the mineral scaffold remains. There is zero risk of transmitting diseases like HIV or hepatitis. It is ethical, safe, and effective.
Xenografts: Usually derived from bovine (cow) bone. It is heated to extremely high temperatures, which removes all organic material. You are left with a clean, porous structure that is almost identical to human bone. It is very popular for sinus lifts (a specific type of graft for the upper jaw).
Alloplasts: These are entirely man-made. They often contain tricalcium phosphate or hydroxyapatite. They are fantastic because there is no limit on supply, and they carry zero ethical concerns for some patients.
Specific Types of Grafting Procedures (H3)
Not every bone graft looks the same. The name of the surgery changes depending on where the bone is missing.
Socket Preservation (Ridge Preservation)
This is the most common and least invasive graft. It happens immediately after a tooth extraction. Instead of leaving the empty hole to heal, the dentist fills the socket with graft material and covers it with a membrane. This prevents the normal bone collapse that happens after an extraction. If your dentist offers this, take it. It saves you time, money, and pain later.
Ridge Augmentation
This is for when the bone has already collapsed. The top of your jaw ridge (where the teeth sit) becomes too narrow or too short. The surgeon cuts the gum, exposes the flat bone, and screws or ties graft material onto the existing bone. Over months, the ridge grows taller and wider.
Sinus Lift (Sinus Augmentation)
This is specific to the upper back jaw (the premolar and molar area). Right above those teeth are your maxillary sinuses—empty air spaces. When those teeth are lost, the sinus often expands downward, eating away the bone. A sinus lift involves lifting the sinus membrane up and placing graft material under it, in the space where bone should be. This creates enough height for an implant.
The Step-by-Step Surgical Experience
Knowing what happens during the surgery reduces fear. Let me walk you through a typical ridge augmentation or socket preservation.
Step 1: Anesthesia and Sedation
You will be completely numb. You might feel pressure but no pain. For anxious patients, oral sedation (a pill) or laughing gas is available. You are awake but deeply relaxed.
Step 2: The Incision
The surgeon makes a small cut in your gum tissue to expose the bony defect.
Step 3: Placing the Graft
The chosen graft material is hydrated (mixed with saline or blood) to form a putty-like consistency. It is packed firmly into the missing area.
Step 4: The Barrier Membrane
Often, a collagen membrane is placed over the graft. This acts like a blanket. It keeps the graft particles in place and prevents your gum tissue (which grows faster than bone) from invading the space. We want bone to grow, not gum.
Step 5: Closing and Stitches
The gum is sutured back into place. The stitches are usually the dissolving type, so you do not need to return to have them removed.
How long does the surgery take?
- Socket preservation: 15–30 minutes.
- Ridge augmentation: 45–90 minutes.
- Sinus lift: 60–120 minutes.
Recovery Timeline: What to Expect Week by Week
Healing from a bone graft is a waiting game. You cannot rush biology. Here is a realistic timeline.
Days 1 to 3 (The “Sore” Phase):
- Mild to moderate swelling. Bruising on the face is possible.
- You will eat soft foods (yogurt, soup, smoothies, mashed potatoes).
- Do NOT spit, use a straw, or smoke. The blood clot needs to stay in place.
- Ice packs on the face for 20 minutes on, 20 minutes off.
Days 4 to 7 (The “Turning Point”):
- Swelling peaks around day 3, then slowly goes down.
- You can switch to warm compresses to increase blood flow.
- You might see small white or gray flecks in your mouth. Do not panic. These are particles of graft material coming loose. It is normal.
Days 10 to 14 (Stitches Out):
- If you have non-dissolving stitches, the surgeon removes them. This is painless.
- The gum tissue should be pink and closed.
- You can slowly return to normal chewing, but avoid the graft site.
Weeks 3 to 12 (The “Quiet” Healing):
- The gum looks healed, but deep inside, the graft is turning into bone.
- You will forget you had surgery.
- Avoid hard or crunchy foods directly on the site.
Month 4 to 9 (Integration Complete):
- The graft is now living bone.
- Your dentist takes a CT scan (3D x-ray) to measure the new bone density.
- You are ready for dental implant placement.
A Critical Note: The grafted area is weaker than natural bone during the first 3 months. After 6 months, it is stronger than the original bone because it is denser.
Pain Management and Medications
Let us be honest: you will feel discomfort, but you will not be in agony. Most patients compare the pain to a moderate tooth extraction or a deep bruise.
- Over-the-counter options: Ibuprofen (Advil/Motrin) is excellent because it reduces inflammation. Acetaminophen (Tylenol) helps with pain but not swelling.
- Prescription options: For larger grafts (hip bone or major sinus lifts), the surgeon may prescribe a mild narcotic for 2–3 days. Most patients do not finish the bottle.
- Antibiotics: You will likely take a week-long course to prevent infection. Finish the entire course, even if you feel fine.
- Antiseptic rinse: A chlorhexidine mouthwash is often prescribed. Use it gently. Do not swish vigorously.
Success Rates and Risks
When performed by a qualified professional, dental bone grafting has a success rate of over 90% . Small grafts (socket preservation) approach 98% success. Large grafts (extensive ridge augmentation) are closer to 85-90%.
Potential Complications (The Honest List)
No surgery is risk-free. Here is what can go wrong, though complications are rare.
- Infection (2-5%): Signs include pus, increasing pain after day 5, fever, or a bad taste. Treated with antibiotics or draining.
- Graft Failure (Non-union): The graft never turns into bone. The body rejects or breaks it down. The only fix is a second graft with different material.
- Membrane Exposure: The protective membrane pokes through the gum. Small exposures heal on their own. Large ones need a second surgery to cover.
- Nerve Injury (Very Rare): Only a risk in the lower jaw near the nerve that supplies the lip and chin. Usually temporary numbness lasting weeks or months.
- Sinus Problems: After a sinus lift, you might feel sinus pressure or a runny nose. Avoid blowing your nose for 2 weeks.
Signs You Need to Call Your Surgeon Immediately
- Bright red blood that fills your mouth (not just pink saliva).
- Swelling that makes it hard to swallow or breathe.
- A fever over 101°F (38.3°C).
- Numbness in your lip that does not go away after the anesthetic wears off.
Cost of Dental Bone Grafting
This is the question everyone asks. Prices vary wildly based on your location, the surgeon’s expertise, and the type of graft.
Here is a realistic range in the United States (without insurance):
| Procedure | Average Cost (Per Site) |
|---|---|
| Socket Preservation (at extraction) | 200–500 |
| Ridge Augmentation (small, 1-2 teeth) | 500–1,200 |
| Ridge Augmentation (large, 3+ teeth) | 1,500–3,000 |
| Sinus Lift (one side) | 1,500–2,500 |
| Sinus Lift (both sides) | 2,500–5,000 |
| Autograft from hip (hospital setting) | 5,000–10,000+ |
Does dental insurance cover bone grafts?
It depends. Medical insurance sometimes covers grafting if the bone loss is caused by trauma, cysts, or tumors. Dental insurance rarely covers grafting just for implants. However, some PPO plans cover 50% of socket preservation after an extraction. Always ask for a pre-determination of benefits.
Payment options: Most clinics offer CareCredit (medical credit card) or in-house financing. Do not let cost stop you from asking about options.
Foods to Eat and Avoid After Surgery
Your diet directly affects your healing speed. Here is a practical guide.
The “Green Light” List (First 2 weeks)
- Dairy: Greek yogurt, cottage cheese, pudding, ice cream (no nuts).
- Soups: Tomato, butternut squash, creamy broccoli (cooled down, not hot).
- Protein shakes: Whey or plant-based. Add peanut butter for calories.
- Soft carbs: Mashed potatoes, oatmeal, cream of wheat, polenta.
- Fruits: Applesauce, smoothies (use a spoon, not a straw), bananas.
- Eggs: Scrambled, soft boiled, or egg salad.
The “Red Light” List (First 4 weeks)
- Crunchy: Chips, nuts, popcorn, hard pretzels.
- Sticky: Caramel, taffy, dried fruit, bagels.
- Spicy: Hot sauce, curry, chili powder (causes irritation).
- Hot temperature: Hot coffee or tea can dissolve the blood clot. Wait 3 days.
- Alcoholic drinks: Alcohol interferes with bone healing. Wait 2 weeks.
- Straws: The suction can pull the graft out of the socket.
Smoking and Bone Grafts: A Hard Truth
I need to be direct with you. Smoking is the number one reason bone grafts fail.
Nicotine constricts your blood vessels. Blood vessels carry oxygen and healing cells to the graft site. Without oxygen, the graft material dies. It does not turn into bone. It becomes a dead piece of material that your body will spit out or infect.
The data: Smokers have a 35-40% higher failure rate compared to non-smokers. For sinus lifts, the failure rate in smokers can be as high as 50%.
What you must do: If you smoke, you need to stop for at least 2 weeks before surgery and 3 months after surgery. Vaping is not better. E-cigarettes still contain nicotine, which constricts blood vessels.
“I tell my patients: a bone graft is an investment. Every cigarette you smoke is like taking a hammer to that investment.” — Dr. James Chen, Oral Surgeon.
Alternatives to Bone Grafting
Not everyone wants or can have a bone graft. Here are the realistic alternatives.
1. Shorter Dental Implants
Technology has advanced. We now have “short implants” that are only 4mm to 6mm long (standard is 10mm to 12mm). If you have moderate bone loss, a short implant might fit without a graft. Ask your dentist about the “Nobel Biocare” or “Straumann” short implant systems.
2. Zygomatic Implants
This is for extreme upper jaw bone loss. Instead of anchoring into the jawbone, the implant anchors into the cheekbone (zygoma). These are very long implants (up to 50mm). Only a handful of specialists perform this. It is expensive but avoids a sinus lift.
3. Traditional Bridge
A dental bridge grinds down the teeth on either side of the gap and places a three-unit crown. It does not require bone grafting. The downside? You damage two healthy teeth, and the bridge does not stop bone loss. The bone under a bridge continues to shrink.
4. Removable Partial Denture
A “flipper” or partial denture clips onto your remaining teeth. It is the cheapest option. However, it is removable, can feel bulky, and accelerates bone loss because it rests on the gums.
Comparison Table: Graft vs. Alternatives
| Option | Requires Graft? | Cost (Relative) | Longevity | Preserves Bone? |
|---|---|---|---|---|
| Implant with Graft | Yes | High | 25+ years | Yes |
| Short Implant | No | Medium-High | 20+ years | Partial |
| Zygomatic Implant | No | Very High | 25+ years | No (uses cheekbone) |
| Traditional Bridge | No | Medium | 10-15 years | No |
| Partial Denture | No | Low | 5-10 years | No |
How to Choose Your Surgeon
Not all dentists perform bone grafts. You need someone with specific training. Here is your checklist.
Option 1: Periodontist (Gum Specialist)
- Best for socket preservation and ridge augmentation.
- Experts in soft tissue and bone.
- Usually the most conservative approach.
Option 2: Oral and Maxillofacial Surgeon
- Best for large grafts and sinus lifts.
- Can perform IV sedation (asleep).
- Best for harvesting bone from the hip.
Option 3: General Dentist with Training
- Fine for small, simple socket preservations.
- Ask how many they have done. Ask to see before/after photos.
- Avoid general dentists offering large ridge augmentations.
Questions to ask during your consultation:
- “How many of these specific grafts do you perform per month?”
- “Do you have a CBCT (3D x-ray) machine in the office?”
- “What is your personal failure rate?”
- “What material do you prefer, and why?”
- “Who manages my care if there is a complication after hours?”
The Connection Between Bone Grafts and Dental Implants
A bone graft is rarely the final step. It is a preparatory step. Here is the full timeline for a typical patient missing a front tooth.
- Month 0: Tooth extraction + socket preservation graft ($300).
- Month 4: CT scan confirms new bone is dense.
- Month 5: Dental implant placement (screw into the new bone).
- Month 8: Osseointegration complete (implant fused to bone).
- Month 9: Abutment (connector) and crown (fake tooth) placed.
- Total time: 9 months.
- Total cost (graft + implant + crown): 4,500–6,500.
Without the graft, the implant would have no bone to hold it. The graft is the hero behind the scenes.
Long-Term Care After a Bone Graft
Once your graft has healed and your implant is placed, you are not “done.” You must maintain the area.
- Daily cleaning: Use a water flosser (Waterpik) around the implant. Regular floss works too, but water flossers are gentler.
- Night guard: If you grind your teeth (bruxism), wear a night guard. Clenching creates forces that can break the graft or implant.
- Regular x-rays: Your dentist should take a periapical x-ray once a year to check the bone level around the implant.
- Professional cleanings: See your hygienist every 6 months. They have special instruments (plastic or titanium scalers) that will not scratch the implant.
Can a bone graft fail years later?
No. If the graft integrates successfully and turns into living bone, it behaves exactly like normal bone. It can only be lost if you develop peri-implantitis (an infection similar to gum disease around the implant). Good hygiene prevents this.
Frequently Asked Questions (FAQ)
1. Is dental bone grafting painful during the procedure?
No. You are completely numb. You will feel pressure, vibration, and noise, but not sharp pain. If you feel pain, raise your hand immediately. The surgeon will add more anesthetic.
2. How long does a dental bone graft take to heal?
The gum heals in 2 weeks. The bone matures in 4 to 9 months. You cannot feel the bone healing. You will only know it is done when the dentist takes an x-ray.
3. Can I get a bone graft and an implant on the same day?
Sometimes. This is called an “immediate implant with simultaneous grafting.” It is only possible if you have at least 50% of the original bone remaining. Most patients need separate surgeries.
4. What happens if I do nothing?
If you need a graft but skip it, you have two options: live with the missing tooth, get a bridge (which damages healthy teeth), or get a denture (which accelerates bone loss). The bone loss will continue slowly over your lifetime.
5. Are dental bone grafts safe for elderly patients?
Yes, age is not a limiting factor. General health is. As long as you are healthy enough for local anesthesia (numbing shots), you are healthy enough for a graft. People in their 80s and 90s receive grafts successfully.
6. Can my body reject a bone graft?
True “rejection” (immune system attacking the graft) is impossible with processed allografts, xenografts, or alloplasts because they contain no cells or proteins to reject. Your body can resorb (break down) the graft if you have a metabolic bone disease or severe infection, but that is not immune rejection.
7. Will my face look different after a bone graft?
No. A bone graft restores the bone you originally had. It does not change your facial shape dramatically. However, if you have had severe bone loss for decades, restoring that bone can subtly improve the support of your lips and cheeks, making you look slightly younger.
Additional Resources
For those who want to dive deeper into peer-reviewed information, here is a trusted external link:
- American Academy of Periodontology (AAP): “Bone Grafts for Dental Implants” – https://www.perio.org/ (Search “bone grafting” in their patient education section).
Conclusion
Dental bone grafting is a safe, predictable, and routine procedure that rebuilds lost jawbone to make dental implants possible. While it adds time and cost to your treatment plan—typically four to nine months of healing—it offers a permanent solution for missing teeth that preserves your facial structure and oral health. With a success rate above 90%, the procedure is well worth considering if your dentist recommends it. Remember: the graft itself is not painful thanks to modern anesthesia, and the recovery is manageable with soft foods and rest.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a licensed dentist or oral surgeon in your location for a personal diagnosis and treatment plan. Individual results vary. The author and publisher are not liable for any actions taken based on the contents of this guide.