Implant vs. Mini-Implant: The Unfiltered Truth About Your Tooth Replacement Options
Losing a tooth feels deeply personal. It changes how you smile in photographs. It changes how you chew a crisp apple on a summer afternoon. It even changes the way you pronounce certain words when you order your morning coffee. You want a solution that feels permanent, stable, and natural. The research leads you down a rabbit hole of dental jargon. Eventually, you land on two competing paths. On one side, you see the traditional dental implant—a robust, time-tested titanium post. On the other side, you see the mini-implant—a thinner, less invasive alternative that promises a faster recovery.
The information available often feels like a sales pitch rather than medical advice. One clinic pushes the “new, needle-free” method, while another insists that “bigger is always better.” Neither of these extreme narratives gives you the full picture. A dental implant and a mini-implant are not identical twins. They are more like cousins, sharing a family resemblance but designed for very different jobs.
This guide strips away the marketing fluff. We will walk together through the gritty details of bone density, surgical drilling, financial breakdowns, and painful failure rates. You will not find artificial filler here. You will find a realistic, honest, and deeply researched comparison. By the time you reach the final paragraph, you will not just understand the difference between an implant and a mini-implant. You will know exactly which road leads to a lifetime of confident chewing and which one might lead to a costly detour.
Setting the Stage: What Does “Tooth Replacement” Actually Require?
Before we draw battle lines between the two devices, let’s look at the battleground itself: your jawbone. Missing a tooth triggers a biological chain reaction. Bone tissue, much like a muscle, needs constant stimulation to stay strong. The roots of your natural teeth provide that workout every time you bite down. Remove the tooth, and the stimulation stops. The body starts resorbing the bone mineral elsewhere, causing the jaw to slowly shrink in width and height.
A successful tooth replacement strategy must fight this shrinkage. It can’t just be a cosmetic mask sitting on top of the gum. It has to anchor into the bone to keep it alive. Both traditional implants and mini-implants achieve this, but the way they distribute force is fundamentally different. Think of a traditional implant as a concrete pylon supporting a bridge. Think of a mini-implant as a steel pin used to stabilize a smaller, lighter structure. The physics of their designs dictate where and when you should use them.
Dentists often use the term “osseointegration.” It sounds complex, but it simply means the bone cells physically attach themselves to the titanium surface. Titanium is biocompatible. Your immune system doesn’t attack it. It treats it like welcome scaffolding. Both implants undergo this process, but the larger surface area of a standard implant generally locks into the bone with a stronger mechanical grip.
There is a common misconception floating around online forums that mini-implants are simply scaled-down versions of regular implants. That is not entirely accurate. The connection mechanism is different. A traditional implant usually features an internal screw chamber where the dentist places an abutment (a connector piece), and finally, a crown covers it. A mini-implant often exists as a single piece of solid metal. The top of the mini-implant, shaped like a ball or square, sticks out of the gum, and the denture snaps directly onto it. This design distinction matters immensely for long-term maintenance.
“The success of osseointegration depends less on the name of the implant and more on the gentleness of the surgical technique and the health of the patient’s blood supply.” – A reflection shared in a journal of implant dentistry.
You should not interpret this as a “one-size-fits-big” narrative. Bigger isn’t universally better if the big item cannot fit. However, smaller isn’t universally more comfortable if it fails to handle the load. Context eats absolute rules for breakfast.
The Architectural Breakdown: Dimensions, Materials, and Core Designs
To make a truly informed choice, you need to understand the physical object going into your jaw. We need to measure things in millimeters. A millimeter might not sound like much, but in dentistry, a difference of 1.5 mm can determine whether an implant shatters the bone or integrates beautifully.
What Defines a Traditional Dental Implant?
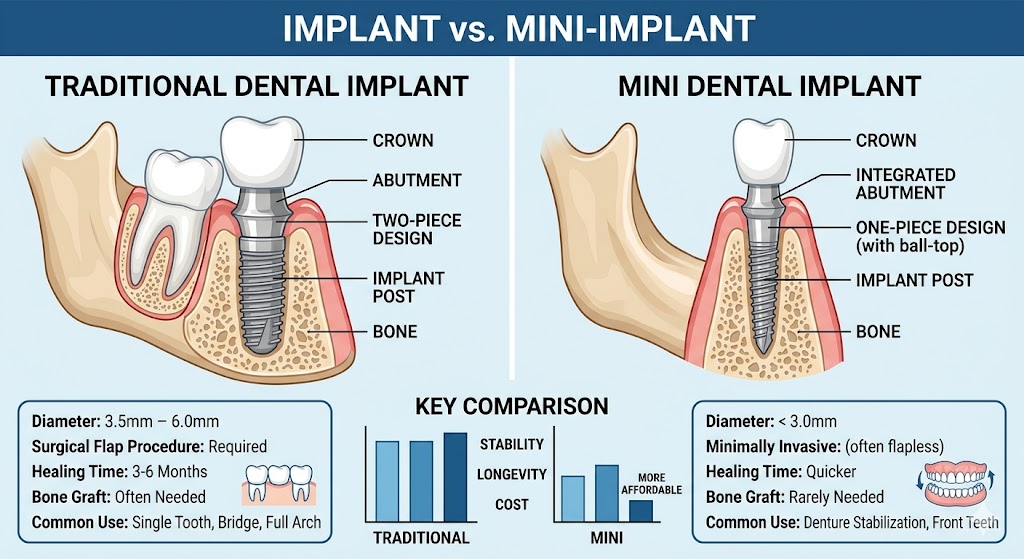
A standard implant consists of two, sometimes three, distinct components. The fixture is the screw that goes into the bone. The abutment is the post that screws into the fixture. The restoration is the fake tooth on top. This modular design allows for a high degree of customization. If a crown cracks ten years later, the dentist unscrews it from the abutment and replaces it without touching the bone-anchored fixture.
Standard implants typically possess a diameter ranging from 3.25 mm to 5.0 mm, occasionally wider for molars. Their length usually sits between 8 mm and 16 mm. The surface is not smooth like a hardware screw. Manufacturers roughen it up at a microscopic level through sandblasting or acid etching. This roughness dramatically increases the surface area. More surface contact equals more bone cells gripping the metal.
The material is medical-grade titanium alloy or, increasingly, zirconia for patients wanting a metal-free option. Titanium remains the benchmark. Its elasticity is relatively close to bone, which prevents stress-shielding. Stress-shielding happens when a material is so stiff that the bone underneath stops feeling pressure and wastes away. Titanium flexes just enough to keep the jawbone exercised.
What Defines a Mini Dental Implant?
A mini-implant (often abbreviated as MDI) is a single-unit device. The post and the abutment are one solid piece of titanium. The dentist cannot separate them. This changes the restorative workflow. Since the top of the implant protrudes through the gum, the restoration (usually a denture with a rubber O-ring housing) snaps directly onto it.
The diameter is drastically thinner, usually clocking in between 1.8 mm and 3.0 mm. Because they are so narrow, they often require a less invasive placement technique. A dentist frequently places them directly through the gum tissue without a scalpel incision. They literally twist them in like a tiny screw through a sheet of drywall, hoping to hit the wooden stud (the bone) perfectly. This “flapless” surgery reduces bleeding and removes the need for stitches.
However, the solid monolithic design presents a problem. The connection between the bone and the implant is not the only weak point. The neck of a mini-implant, where the metal transitions from the rough bone surface to the smooth gum surface, is thin. It measures barely 1.8 mm across. This is the spot where bending forces concentrate. Imagine holding a paperclip and bending it back and forth repeatedly. It snaps eventually. Metal fatigue is a real threat for ultra-thin components under constant chewing loads.
A Quick Note on Material Differences: Most mini-implants are titanium alloy, specifically a tougher grade (Ti-6Al-4V) to compensate for the smaller diameter. Yet, even the strongest alloy cannot defeat the laws of physics. A thinner rod bends more easily than a thicker rod of the same material. This is not a defect; it is geometry.
Comparison Table: Physical Specifications
| Feature | Standard Implant | Mini-Implant |
|---|---|---|
| Diameter Range | 3.25 mm – 6.0 mm | 1.8 mm – 3.0 mm |
| Design Structure | Two-piece (Fixture + Abutment) | One-piece (Solid Monolithic) |
| Connection Type | Internal Hex/Conical Connection | O-ball/Square/Rubber O-ring head |
| Surface Texture | Highly roughened (etched/grit-blasted) | Moderately roughened or machined |
| Surgical Entry | Flap surgery (tissue reflection) | Often Flapless (transmucosal) |
| Invasiveness | Moderate (may require grafting) | Low to Minimal |
Stability, Bone, and the Crucial Question of Width
The biggest deciding factor rarely revolves around the dentist’s preference. It revolves around the hard numbers of your computed tomography (CT) scan or 3D X-ray. Bone anatomy is uncompromising. If the width of your jaw ridge measures 5 mm or more, a traditional implant fits. If the ridge has collapsed to a razor-thin edge of 3 mm or less, a standard implant simply cannot fit without surgical augmentation.
This is where mini-implants historically entered the spotlight. Dentists marketed them as the “no-bone-graft” solution. Indeed, you can often thread a 2.4 mm screw into a ridge that looks hopelessly narrow on an X-ray. This appears to be a miracle cure for denture wearers who have suffered severe bone loss over decades. Upper dentures, in particular, often cause extreme shrinkage of the premaxilla (the front upper jaw). A standard implant here requires extensive bone grafting from the hip or cadaver sources, adding months of healing and thousands of dollars.
But placing an implant simply because it “fits” is a dangerous logic. The question is not just “Can we fit it?” but “Will it survive the torque of the patient’s lifestyle?” Bruxism (teeth grinding) generates hundreds of pounds of lateral force. A thick implant distributes this force across a large bone volume. A mini-implant focuses the same force on a razor-thin cross-section. The bone surrounding a mini-implant experiences high-stress peaks. Over time, this stress can exceed the physiological limit of bone remodeling. The bone cells die, the implant loosens, and you lose the anchor.
Real Talk: Think of a stiletto heel versus a snowshoe. A standard implant is the snowshoe. It spreads the pressure wide. A mini-implant is the stiletto. It penetrates easily and supports weight, but on a soft surface (or under extreme pressure), it punches through. If you clench hard, mini-implants may not forgive you.
The Surgical Journey: The Chairside Experience
Dental anxiety often steers patients toward the “mini” option. The word “surgery” triggers cortisol spikes. The promise of a “non-surgical” or “minimally invasive” solution feels like a warm blanket. Let’s dissect exactly what happens in both procedures so you can differentiate between psychological comfort and physical reality.
The Standard Implant Surgery Protocol
This is a staged surgical event. In a perfect, textbook scenario, the process follows three phases over four to six months.
First, the dentist administers profound local anesthesia. You feel fully numb, but you remain awake. The dentist makes a precise incision in the gum to peel back a flap of tissue, exposing the raw bone underneath. You might hear the sound of the drill. A series of progressively wider drill bits carefully prepare a hole in the bone. Copious sterile saline water cools the site to prevent heat necrosis (bone death from friction). The implant fixture screws in slowly until it sits flush with the bone. The dentist places a cover screw on top, and stitches the gum shut.
You wait. For the next 3 to 6 months, you do not wear a tooth on that implant. The bone grows into the threads. This “submerged” healing protects the implant from the micromovement that occurs if you accidentally bite on it. Micromovement is the number one killer of osseointegration.
After the waiting period, the dentist makes a tiny incision to expose the buried implant and attaches a healing abutment. The gum shapes itself around it for two weeks. Finally, impressions create the final crown. The multi-step nature ensures maximum predictability. The success rate for this method, in healthy patients, hovers around 96-98% according to longitudinal data published by the American Academy of Implant Dentistry.
The Mini-Implant Procedure: Speed and Simplicity
The mini-implant procedure often happens on the same day as the tooth restoration, hence the catchy marketing term “Same-Day Teeth.” This immediacy solves a huge emotional problem: you don’t leave the office with a gap.
The dentist identifies the precise entry point using a surgical guide or direct visualization. A needle delivers anesthetic. No scalpel touches your gum. The dentist takes a needle-thin drill and punches a starter hole directly through the dense gum tissue and into the outer layer of bone. Then, they take the mini-implant, loaded on a finger driver or a handpiece, and manually screw it in. They screw it until the torque resistance reaches a sweet spot—tight enough to achieve primary stability, but not so tight that it strips the bone threads. The ball-top of the implant sits exposed in the mouth.
Here is the critical moment. Unlike the standard implant, which hides under the gum for months, the mini-implant stands proud in the battle zone immediately. The tongue, cheek, and food debris will hit it constantly. If the denture or crown attaches to it right away, the risk of micromovement skyrockets. Some protocols allow immediate loading, but only if a rigid splinting bar connects multiple mini-implants together to create a “tripod” effect, resisting movement through numbers.
“Immediate loading is not a free pass. It demands a strict mechanical formula. Four splinted mini-implants can do the job of one resting standard implant, but only if they are placed absolutely parallel and the bite force is perfectly balanced.” – A clinical observation on immediate load protocols.
The absence of stitches means zero post-operative “tightness,” but you will feel the metallic protrusion against your lip. For some, this causes a persistent foreign-body sensation that takes weeks to neurologically desensitize.
Pain Comparison: A Sober View
Marketers often claim mini-implants cause “no pain.” This is a distortion. Needle delivery of anesthetic hurts equally for both. The bone drilling causes a vibration sensation. Since mini-implants bypass the scalpel cut, there is no stinging sensation from the incision. Post-operatively, a standard implant site feels bruised and swollen for roughly 48 hours because the tissue was reflected. A mini-implant site usually exhibits zero swelling. However, if the mini-implant places too much pressure on the thin tissue collar, it can cause a dull ache as the tissue stretches. Neither option is a walk in the park, but the standard implant is objectively more taxing on the body’s soft tissue healing response.
Bone Grafting: The Expensive Dealbreaker
Here lies the elephant in the room. When you sit in the consultation chair and the dentist says, “You need a bone graft,” the mental clock starts ticking. A graft adds months of healing. It adds significant cost. It adds a second surgical site, usually the roof of your mouth, your hip, or processed donor bone. Suddenly, the mini-implant—a device that can often skirt around the need for grafting—looks impossibly attractive.
Can a mini-implant truly cheat biology? Yes and no.
If the bone volume is simply narrow horizontally, a long, thin mini-implant can anchor in the basal bone deeper down. Basal bone is the dense, core jawbone that resists resorption. Standard implants typically rely on the alveolar bone (the ridge), which vanishes first. Mini-implants acting as “root-form” screws in the basal bone can bypass the deficient ridge entirely.
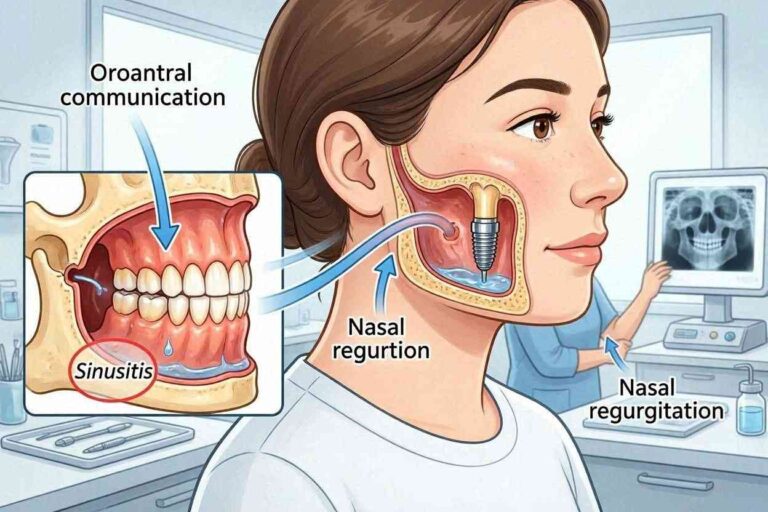
However, if the bone is vertically deficient—meaning the sinus cavity in the upper back jaw has dropped, or the nerve canal in the lower jaw sits dangerously high—the mini-implant simply lacks enough length to stabilize. The longest mini-implant you can safely use is about 15 mm. If your available bone height measures only 6 mm, neither implant works without a grafting procedure. A sinus lift pushes the sinus membrane up and packs bone beneath it. Bypassing this with a short mini-implant often results in perforation of the sinus floor and chronic sinus infections.
Critical Boundaries for Bone Volume
| Bone Condition | Standard Implant Feasibility | Mini-Implant Feasibility |
|---|---|---|
| Width > 5 mm | Excellent; no graft needed. | Possible, but unnecessary. |
| Width 3 – 4.9 mm | Usually requires ridge-split/bone graft. | Often feasible without grafting. |
| Width < 3 mm | Requires block bone graft. | May fit, but high risk of gum recession. |
| Height > 12 mm | Ideal. | Ideal. |
| Height 8 – 11 mm | Short implants (8mm) used. | Most mini lengths work. |
| Height < 8 mm | Requires sinus lift/nerve transposition. | High failure rate; limited by length. |
You must resist the urge to demand a mini-implant solely to avoid a recommended graft. Skipping a necessary graft can lead to an implant that thread-lifts the sinus membrane or compresses the mandibular nerve. The former causes infection; the latter causes permanent lower-lip numbness. That is a devastating price to pay for saving three months of healing.
The Stability Paradox: Why Smaller Isn’t Always More Comfortable
Let’s examine a subtle concept that rarely makes it into the glossy pamphlets: denture stability. If you are exploring these options, you likely hate your loose lower denture. You want it to snap down tight. The marketing logic assumes that an implant is an implant, and any anchor will hold the denture still. Unfortunately, physics tells a different story.
A traditional implant with a Locator abutment uses a nylon insert in the denture that snaps onto a metal abutment. The abutment diameter is usually around 3.5 mm to 4.5 mm. This large surface area creates a solid snap. It resists the “floating” motion.
A mini-implant head uses a rubber O-ring inside the denture. The head is roughly 1.8 mm to 2.5 mm. The retention force is weaker. It feels like clicking a pen, not sealing a water bottle. For a brand-new patient, this feels miraculously tight compared to a floating denture. However, the O-ring wears out. The rubber fatigues under saliva and constant insertion/removal. A patient with strong cheek muscles or a heavy bite will find that the denture begins to “rock” slightly on the O-rings after just six months. This rocking levers the mini-implant back and forth.
Standard implants rarely rely on rubber O-rings for retention. They use high-retention nylon inserts (like the Locator system) or are screwed solidly onto bars. The connection is a friction-fit of a larger circumference. This doesn’t just keep the denture in; it restricts lateral tipping. For a lower denture that sits over the tongue, a metal bar supported by four standard implants provides nearly 100% stability, as if the patient had permanent teeth again.
“You aren’t just replacing teeth. You’re creating a structural frame to resist the tongue. The tongue is a powerhouse muscle that never tires. It will defeat a weak mechanical connection every time.”
Prosthetic Options: What Are We Actually Screwing In?
The final tooth matters. We need to distinguish between the implant and the restoration it supports. The restoration dictates the load.
Single Tooth Replacements
Here, the verdict leans heavily toward the standard implant. The dental community universally agrees that replacing a single molar or premolar with a mini-implant is a high-risk gamble. Chewing forces on a single back tooth can exceed 200 pounds per square inch. A standard implant distributes this via a thick abutment screw. A one-piece mini-implant, in contrast, places an artificial crown directly on a 2.4mm post. The lever arm is extreme. Every chew flexes the neck of the mini-implant. Microscopic gaps open at the gum line, inviting bacteria. Within 12 to 18 months, many single-tooth mini-implants placed in high-stress areas develop mobility, or the metal fractures outright.
Mini-implants for single anterior (front) teeth have a slightly better prognosis because the lateral forces are lower. Yet, the aesthetic challenge arises. The gum tissue around a 2.5mm platform often recedes, creating a “black triangle” or exposing the metal thread. A standard implant uses a wider platform that better supports the gum papilla, yielding a more natural cosmetic profile.
Full Arch Rehabilitation (The All-on-X Concept)
The “All-on-4” protocol revolutionized full-mouth restoration. It uses four standard, angulated implants to support a full bridge of teeth immediately. Can mini-implants replicate this? No. Mini-implants are not designed to support a rigid, screw-retained bridge of twelve teeth. The torque required to unscrew a bridge would unscrew the mini-implant from the bone.
Mini-implants support removable overdentures. The patient pops the denture out at night. This is an important lifestyle distinction. A standard implant bridge is “fixed.” Only the dentist takes it out. A mini-implant overdenture is a removable appliance. You clean it in a glass of water. This distinction dictates your hygiene protocol and your psychological satisfaction. Some patients specifically want the teeth “screwed in permanently.” They hate the ritual of removing teeth. Mini-implants cannot offer that permanent fixed feeling.
List: Ideal Scenarios for Standard vs. Mini Restorations
- Standard Implant Ideal For: Single molars, fixed bridges, full-arch permanent porcelain bridges.
- Standard Implant Ideal For: Patients with bruxism who cannot control grinding.
- Standard Implant Ideal For: Sites with ample bone where grafting is not a financial or medical barrier.
- Mini-Implant Ideal For: Stabilizing a loose lower denture when bone width is severely deficient.
- Mini-Implant Ideal For: Medically compromised patients who cannot undergo extensive grafting surgery.
- Mini-Implant Ideal For: Temporary support during the healing of a standard implant (transitional implants).
- Mini-Implant Ideal For: Upper denture retention where sinus grafting is strictly refused.
The Financial Reality: More Than Just a Price Tag
If you look at a price chart in a dental office, the numbers seem clear. A mini-implant might cost $500 to $1,500. A standard implant and crown might cost $3,500 to $6,000. The math appears simple: four mini-implants cost less than one standard implant. This is dangerous accounting. You must calculate the long-term maintenance.
The Upfront Costs
The lower cost of the mini-implant comes from the reduced surgical time (no flap, no sutures) and the less expensive hardware. The solid titanium screw is cheaper to manufacture than a complex two-piece fixture with a precision internal hex. Sedation costs are often lower. Bone grafting costs vanish.
A standard implant’s upfront price includes the CT scan, the surgical guide, the fixture, the healing abutment, the impression coping, the custom abutment, and the porcelain crown. It is a stack of high-precision components.
The Maintenance Trap
Here is the unvarnished truth about mini-implant maintenance: the O-ring failure cycle. The little rubber rings inside the denture that snap onto the ball-heads of the mini-implants wear down. They are a consumable item, much like brake pads on a car. You will visit the dentist every 6 to 12 months to swap these rings. Some clinics charge $50 to $100 per ring. For four implants, that’s a recurring $400 annual expense.
Furthermore, the threaded mini-implant’s head is soft compared to the opposing porcelain teeth. Over the years, the metal ball wears down, flattening out. Once a mini-implant head loses its spherical shape, retention drops catastrophically. You cannot “replace the head” because it’s one solid piece. The entire mini-implant must be unscrewed from the bone, which often requires trephination (cutting a core of bone around it). You start from zero.
A standard implant’s crown may chip or fracture. The dentist simply unscrews the screw-retained crown and orders a new one. The fixture in the bone stays untouched. The internal abutment screw may fracture under overload, acting as a “mechanical fuse.” The dentist retrieves the broken screw and replaces it. The infrastructure of the bone-level implant often lasts 25 years or more, with prosthetic repairs handled chairside.
Comparison Table: Long-Term Economics
| Expense Category | Standard Implant | Mini-Implant |
|---|---|---|
| Initial Surgical Fee (per unit) | High ($1500 – $3000) | Low ($400 – $1000) |
| Prosthetic Cost (Crown/Denture) | High (Custom CAD/CAM) | Moderate (Denture housing/O-ring) |
| Bone Grafting Necessity | Often required | Rarely required |
| Annual Maintenance | Low (Check-up/exam) | High (O-ring replacements) |
| 10-Year Component Failure Risk | Low (Abutment screw) | High (Metal fatigue/head wear) |
| Insurability | Often partially covered | Often classified as a “retentive aid” |
You should look at mini-implants as a lease on stability rather than a purchase of permanence. They buy you quality of life now at a lower entry fee, but the subscription fees continue for life. Standard implants are the capital investment. The upfront capital is painful, but the long-term interest is minimal.
Failure Modes: How Things Go Wrong
Every dental device fails. The difference lies in how they fail, and what the salvage options look like.
The Ailing Standard Implant
Standard implant failure usually declares itself within the first year (early failure) or after years of neglect (peri-implantitis). Early failure stems from poor surgery, overheating the bone, or a genetic lack of healing response. The implant simply spins in the bone. The dentist removes it easily, often without removing much bone. After a healing period, they place a wider implant in the same site. The salvage rate is high because the original osteotomy site was specific.
Peri-implantitis is the late-stage monster. It is gum disease around the implant. The rough threads become exposed to the oral cavity. Bacteria cause crater-like bone loss. This looks like a moat around the post. Treatment involves opening the gum, disinfecting the threads, and grafting bone. If the bone loss is extreme, the implant must be cut out. Removing a fully integrated standard implant is a brutal procedure requiring a trephine bur to core out the entire implant-bone block. It leaves a massive defect.
The Failing Mini-Implant
Mini-implants fail differently. Because they are thin, the body sometimes treats them like a splinter and exfoliates them. The gum gets red around the tiny head. The implant slowly “unscrews” itself from the bone via cyclic micromovement. A patient often reports, “I felt it wiggling, then I licked it, and it just spun out.” Surprisingly, this atraumatic self-ejection is a blessing. The bone defect left behind is tiny. It heals in weeks. Placing a new mini-implant in the adjacent location is simple.
The true disaster arises when a mini-implant fractures. If the head snaps off leaving the threaded body buried in the jaw, retrieving it is a nightmare. It is too thin to grab with a driver. The dentist must drill around it, destroying a substantial cylinder of bone, and potentially severing the nerve. This is a catastrophic failure mode unique to the one-piece design.
Important Medical Note: Any implant, regardless of size, placed in the upper arch near the sinus can migrate into the sinus cavity if primary stability is lost. This happens more frequently with mini-implants because they lack the macro-locking threads of a standard implant to prevent gross migration. Retrieval from the sinus requires an ENT surgical referral.
Softer Tissues, Harder Problems: The Gum Aesthetic Challenge
We often obsess over bone and leave gum tissue as an afterthought. But you do not see the bone when you smile. You see the crown and the pink gum framing it. The transition zone—the “emergence profile”—determines if the tooth looks real or like a white chicklet stuck in plastic gum.
Standard implants, particularly those placed with a two-piece system, allow for customization of the emergence profile. A healing abutment with a wide, scalloped shape molds the gum. The final crown emerges from the gum naturally, with a diameter mimicking a natural tooth. The gum hugs the crown tightly.
A mini-implant’s one-piece body forces a specific diameter at the gum line. The neck of the implant rarely exceeds 2.5 mm. The restoration (the false tooth) must suddenly flair out from this narrow base to form a tooth size of 8 mm to 10 mm. This creates an undercut. Food traps form. The gum attaches to the smooth collar via a “junctional epithelium” barrier, but this barrier is weak due to the tiny circumference. Recession is common. The silver metal collar becomes visible under the lip. For lower dentures, this doesn’t matter because the acrylic flange covers it. For a single anterior tooth, it is an aesthetic death sentence.
List: Relative Contraindications
- Do not choose a single mini-implant in the aesthetic zone if you have a high lip line.
- Do not choose a mini-implant if you have uncontrolled type II diabetes or a heavy smoking habit (micro-vascularity is already compromised; tiny implants need pristine blood flow).
- Do not choose a standard implant if you have a severe bleeding disorder that prevents surgical incisions.
- Do not choose a standard implant if you suffer from severe vasovagal syncope and cannot endure longer surgical chair times.
Decision Tree: Which Path Fits Your Mouth?
Making this choice involves a logical flowchart rather than a gut feeling. Let’s strip it down to three clinical starting points.
Scenario A: The Single Missing Tooth
You have one gap. The adjacent teeth are virgin and healthy. You do not want a bridge. The X-ray shows 8mm of bone width and 12mm of height. The answer is unequivocally a standard implant with a custom ceramic crown. It mimics nature. It lasts decades. A mini-implant here is biological corner-cutting that ends with a fractured post and an emergency extraction.
Scenario B: The Severely Resorbed Edentulous Lower Jaw
You have been wearing a lower denture for 25 years. It floats. You gag when it lifts. The bone is 2.5 mm wide. A standard implant requires a major bone graft from your hip, costing $15,000 and a year of healing. You are 82 years old. You refuse the surgery. In this instance, four to six mini-implants placed strategically, splinted with a rigid metal bar in the denture, or kept as single O-ring anchors, will transform your life. It will likely fail in some respects within 5 years, but at 87 years old, the risk-benefit ratio is overwhelmingly positive.
Scenario C: The Full Upper Arch
The upper denture covers the palate. It ruins the taste of food. You want it gone. The sinus cavities hang low. Avoiding a sinus graft is your priority. While mini-implants can retain an upper denture, the bone here is often so soft (Type III or IV bone) that mini-implants spin out. The standard “All-on-4” solution uses angulated posterior implants to avoid the sinus by placing them in front of it, not by bypassing it with thin metal. This scenario heavily favors standard implants, even if it means limited grafting.
“Preserving bone is a long game. The younger you are, the larger the implant diameter should be. You need spare bone for the inevitable re-operations later in life.”
Pros and Cons Quick Reference
| Standard Implant | Mini-Implant | |
|---|---|---|
| Pros | Highest survival rate (96%+); Restores full chewing force; Modular repairs; Aesthetic gum shaping; Life-long fixed solution. | Minimally invasive surgery; No grafting needed; Immediate loading; Lower upfront cost; Can be placed by general dentists. |
| Cons | Higher surgical cost; Requires healing period; Bone grafting often necessary; Invasive post-op recovery. | Higher long-term maintenance; Risk of metal fatigue; Limited to dentures/small crowns; Gum recession exposing metal; Less stability in soft bone. |
Material Science: The Biocompatibility Angle
A small subset of patients presents with a titanium allergy. Titanium is often labeled inert, but lymphocyte transformation tests reveal sensitivities in roughly 0.6% of the population. For these patients, a standard zirconia ceramic implant becomes the preferred path. It is white, one-piece (usually), and metal-free. Mini-implants do not exist in a ceramic format. The physics of zirconia don’t allow for a 2mm diameter screw that can handle chewing. If you are allergic to metals, mini-implants are a dead end. You must go with standard-diameter ceramic implants or abandon implants entirely.
Additionally, the galvanic corrosion potential exists. Patients who have gold crowns interacting with a titanium mini-implant head rarely notice it, but the electrical current generated in saliva can occasionally cause a metallic taste or a “battery effect” discomfort. Standard implants sit deeper and interact less with surface metals.
The Psychosocial Factor: Acceptance of an Appliance
There is a profound psychological difference between a fixed prosthesis and a removable one. Some patients feel “disabled” by removable teeth. They hate the private ritual of removing them. They feel old. The mini-implant path, being predominantly associated with snap-on dentures, forces the continuation of that ritual. You will still take something out of your mouth and scrub it. Even if it stays tight while eating, the nighttime removal confirms the absence of natural teeth.
The standard implant route, via the fixed hybrid bridge or single crowns, allows the “implant” to behave exactly like teeth. You brush them. You floss them. You sleep with them. You forget they are fake. For mental health and confidence, this fixed solution often offers a superior quality of life return on investment, provided the bank account can absorb the blow.
The “Same-Day” Marketing Gimmick
You will see advertisements for “Teeth in a Day” using both standard and mini-implants. Mini-implants naturally fit this narrative because they achieve primary stability through mechanical threading into dense bone, allowing immediate snapping of a denture. However, immediate loading places the healing interface at risk. A systematic review often cited in evidence-based dentistry confirms that immediate loading of mini-implants supporting overdentures shows high survival, but lower “success” when using strict criteria (no bone loss, no bleeding). The survival vs. success distinction matters. An implant might stay in the mouth (survival) but lose 1.5 mm of bone around it (failing success criteria). That bone loss eventually leads to the implant threading becoming exposed, leading to a chronic infection.
If a dentist loads a mini-implant immediately, they must protect it. The denture must not rock. The bite must be balanced perfectly. You need a rigid pickup of the O-ring housings in the denture base using a hard chairside reline material. Do not let anyone simply retro-fit your old floppy denture onto new mini-implants without a rigid lock. That floppy fit creates a rocking horse effect that pounds the implants until the bone bleeds.
“A loose denture on a mini-implant is more destructive than no implant at all. It converts a static problem into a dynamic jackhammer.”
A Deeper Look at Surgical Trauma and Bleeding
Standard implant flap surgery sounds scary. Indeed, reflecting the periosteum (the connective tissue layer over bone) causes a biological insult. The body responds with swelling and inflammation. The healing cascade involves a fibrin clot, granulation tissue formation, and finally epithelial closure. Patients on blood thinners (aspirin, Plavix, Warfarin, Eliquis) pose a risk. Stopping blood thinners is often dangerous. Here, the flapless nature of mini-implants shines. No flap means almost zero surgical bleeding. Dentists can often place mini-implants without modifying the patient’s anticoagulant therapy. This is a massive safety advantage for the elderly cardiac patient.
Standard implants can also be placed flaplessly using guided surgery (a 3D-printed template), which minimizes bleeding. Yet, the required osteotomy size for a 4.0 mm implant is significantly larger than for a 2.0 mm mini, meaning the bone bleeding is inherently higher.
Maintenance: Keeping the Investment Alive
Regardless of what you choose, your home care must be immaculate. The enemy is plaque. Peri-implant mucositis (inflammation of the gum around the implant) is reversible. Peri-implantitis (loss of bone) is difficult to arrest.
For a single standard implant, you floss it like a natural tooth. You might use a water flosser. For a mini-implant overdenture, you must clean the O-ring housings meticulously. Food debris cakes around the little metal heads. You must brush the exposed implant heads with a soft brush and non-abrasive gel toothpaste. You must soak the denture overnight in a cleaning solution. The discipline is higher. Many mini-implant failures arise from the patient’s inability to clean the complex geometry of the snap system. The tissue grows over the head (hyperplasia) because the rubber O-ring acts like a chronic irritant. This overgrowth requires laser removal.
Integrating the Article’s Core Messages
The comparison between a traditional implant and a mini-implant is not a battle of superiority. It is a diagnostic puzzle. You have a specific volume of bone, a specific budget, a specific tolerance for surgery, and a specific aesthetic demand. These variables shift the recommendation. Do not fall for the trap of online “vs.” battles where one side declares victory. The winner is the implant that fuses to your bone and stays there for the rest of your life without causing pain.
You saw the dimensional differences. A 4.7 mm wide screw offers a mighty foundation. A 2.2 mm screw offers a biological shortcut. Shortcuts sometimes work beautifully, especially in the aged, narrow jaw where grafting is a medical hurdle too high. Shortcuts fail miserably in the young, single-tooth gap where eating a steak is a non-negotiable life requirement.
The financial saw cuts both ways. The mini-implant is cheap today, expensive tomorrow due to the relentless wear of rubber O-rings. The standard implant is a financial gut-punch today, but it may just be the last money you ever spend on that tooth.
Conclusion
Selecting between a traditional implant and a mini-implant comes down to the width of your bone and the intensity of your bite force, not just the price tag. A standard implant provides a permanent, modular foundation built to mimic a natural tooth’s load-bearing capacity for decades, whereas the mini-implant offers a clever, minimally invasive lifeline for shrinking jaws that cannot handle major grafting. Your final choice must balance the surgical reality of your anatomy against the psychological weight of how you want to live—fixed and forgettable or removable and meticulously maintained.
Frequently Asked Questions
Can a mini-implant support a single back tooth like a molar?
While technically possible, placing a single mini-implant to replace a molar is a high-risk strategy. The chewing forces on back teeth are immense, and the thin diameter of a mini-implant creates a weak point where the metal can fracture or the surrounding bone can fail. Most reputable clinicians consider standard-diameter implants the standard of care for single molars. If you choose this path, you are accepting a significantly higher chance of mechanical failure.
How long does a mini-implant truly last compared to a standard implant?
The survival rate of standard implants often exceeds 25 years with minimal maintenance. Mini-implants, due to their design and reliance on rubber O-ring retention, typically have a predictable stable lifespan of 5 to 10 years before the hardware or the prosthetic components require significant replacement. The implant itself might stay in the bone, but the retention head wears down, rendering it useless for holding a denture.
Will my medical insurance cover any of these procedures?
Medical insurance rarely covers standard dental implants unless the tooth loss resulted from a traumatic accident or cancer surgery. Dental insurance often covers a percentage of a standard implant crown, usually capped at a low annual maximum. Mini-implants frequently get classified as a “dentures/retentive procedure,” which might qualify for the dental insurance deductible for dentures, but this varies widely. Always check your specific policy for exclusions regarding “minis.”
Does it hurt more to have a mini-implant removed?
The removal of a mini-implant is usually less traumatic if it has already loosened. Since it is thin, it often unscrews with minimal resistance. However, if a mini-implant has fractured or integrated deeply, the removal requires a trephine drill to cut a bone core around it. This can cause a more significant bone defect. Standard implant removal is almost always a surgical event requiring bone drilling, but the well-defined internal screw channel allows for easier retrieval of broken pieces.
I am a heavy smoker. Is one option better for me?
Smoking constricts blood vessels and severely impairs oral healing. Both procedures suffer a higher failure rate in smokers. However, the larger surface area and thicker bulk of a standard implant give it a slightly better chance of resisting the toxic effects of nicotine compared to the thin, delicate integration interface of a mini-implant. If you cannot quit, a standard implant is marginally safer biologically, assuming a bone graft is not required (as grafting fails heavily in smokers).
Additional Resource:
For a visual breakdown of the molecular process of osseointegration, visit the American Academy of Implant Dentistry’s patient education library. AAID Patient Resources
Disclaimer:
This article is provided strictly for informational and educational purposes. It does not constitute medical advice or a diagnosis. The content within is not intended to replace a professional dental examination, nor does it establish a doctor-patient relationship. Always consult a licensed implant dentist or oral surgeon regarding your individual medical history and dental condition. Treatment results vary significantly based on anatomy, hygiene, and lifestyle.