Osteoporosis and Dental Implants: A Complete, Realistic Guide
Losing a tooth is a deeply personal experience. It affects how you smile at a friend, enjoy a family dinner, or feel about yourself in a quiet moment. The idea of restoring that gap with a permanent, natural-feeling dental implant brings a wave of hope. But if you also live with osteoporosis, that hope can quickly mix with worry. You start asking yourself, “Is this even possible for me? Will my bones hold the implant?”
You are not alone in this question. Millions of people manage osteoporosis, a condition that silently weakens bones, while also facing tooth loss. The relationship between these two realities is not a closed door. It is a conversation that requires knowledge, careful planning, and an honest look at what modern dentistry can achieve. This guide walks you through every aspect of that conversation. We will leave no stone unturned, giving you a realistic picture of the journey, the risks, the incredible successes, and the moments when an alternative path might be wiser.
We will not offer false promises. Instead, we provide a clear, friendly, and deeply researched roadmap to help you navigate your options. By the time you finish reading, you will understand the science, the surgical adjustments, the healing timelines, and the questions to ask your dentist. Let’s begin this journey together, with clarity and confidence.
Understanding the Foundation: Your Bones and Implants
Before diving into the specific challenges and solutions, let’s build a solid foundation of understanding. Think of a dental implant like a house. The visible crown is the roof, and the implant post buried in your jaw is the foundation. For a house to stand for decades, its foundation must be deep, solid, and stable. This exact principle applies to your mouth.
What Exactly Happens with Osteoporosis?
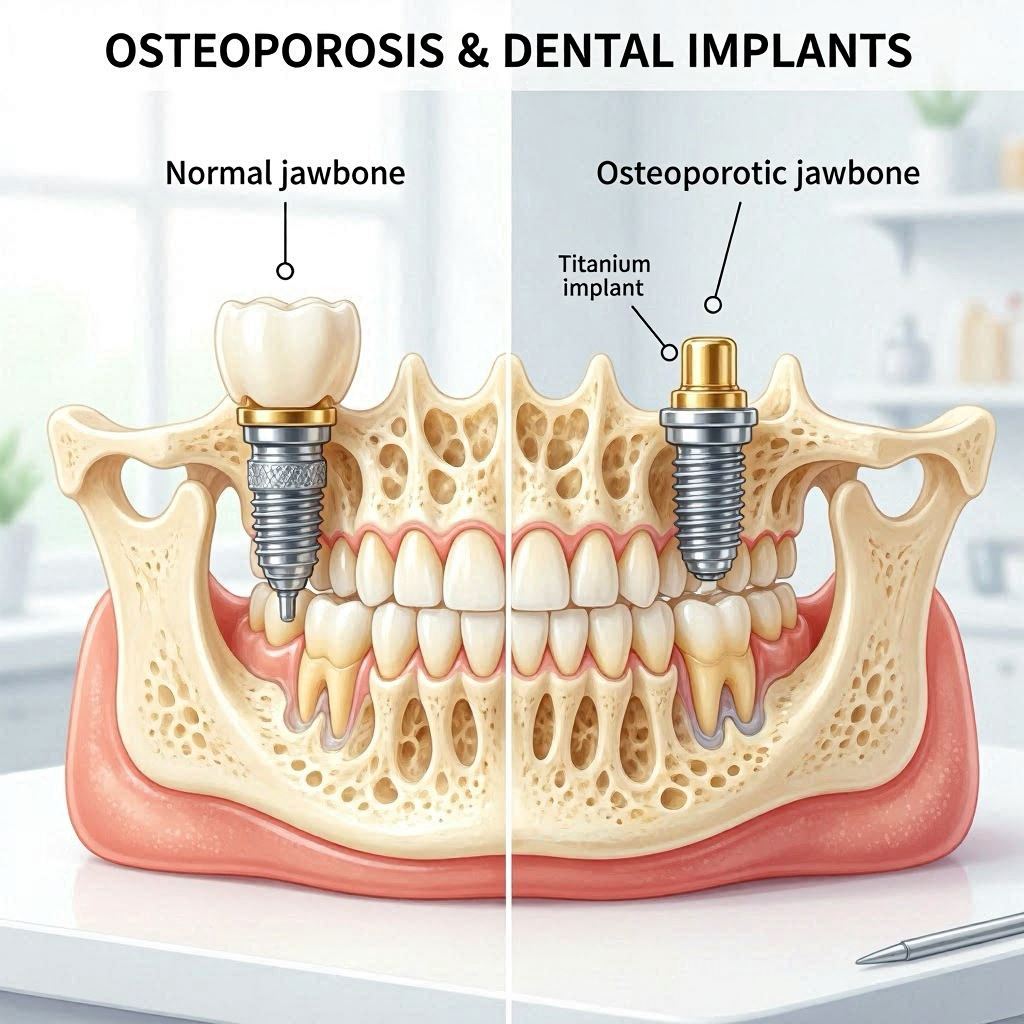
Osteoporosis translates literally to “porous bone.” Under a microscope, a healthy bone looks like a dense honeycomb. In a person with osteoporosis, the holes and spaces in this honeycomb become much larger. The bone loses its density and mass. It becomes fragile, like a piece of driftwood that looks solid on the outside but crumbles under pressure.
This process is silent. You don’t feel your bones getting weaker. For many, the first sign is a fracture from a minor bump or fall. The condition affects the entire skeleton, but we will focus on a specific area: your jaws. The jawbones, the maxilla on top and the mandible below, are the very ground upon which we build a dental implant. They anchor your natural teeth. When teeth are lost, the jawbone in that spot begins a slow process of resorption, shrinking away like an unused muscle. Osteoporosis can accelerate this natural decline.
A Dental Implant’s Greatest Need
An implant is not simply a screw placed into the gum. It is a biocompatible titanium post surgically inserted into the living bone. The magic of the procedure is a process called osseointegration. This is the structural and functional connection between living bone and the surface of a load-bearing artificial implant.
The bone cells, called osteoblasts, grow directly onto the titanium surface, locking the implant in place as if it were a natural tooth root. This process demands two things from the body: enough bone volume to surround the implant and a healthy biological environment for new bone growth to occur. When you have osteoporosis, the quality of that biological environment becomes the central question. The bone may be less dense, and its ability to heal and lock the implant can be compromised. But “compromised” does not mean “impossible.” It changes the rules of the game, and you need to know the new rules.
The Direct Impact of Osteoporosis on Dental Implant Success
Let’s address the most pressing worry. Does having osteoporosis mean an implant will fail? The honest answer is no, but it requires a more nuanced look at your individual health. A large body of research now gives us a realistic picture, moving beyond the old blanket statement that osteoporosis is a contraindication for implants.
Primary and Secondary Stability: The Two-Phase Hurdle
To understand success, you must understand the two critical phases of healing.
The first phase is primary stability. This is the immediate, mechanical grip of the implant in the bone right after surgery. Picture a wood screw being driven into a piece of wood. If the wood is dense oak, the screw bites tightly and is hard to wiggle. If the wood is soft pine, the screw may spin loosely. In your jaw, the surgeon achieves primary stability when the implant is firmly anchored by the cortical bone, the hard outer layer of your jaw, even before any healing begins. In osteoporotic bone, achieving this initial tight fit is the first big challenge. A loose implant at day one has a much higher risk of failure.
The second phase is secondary stability, which is the biological healing we mentioned: osseointegration. After the implant is placed, the surgical trauma triggers a healing cascade. The body removes any damaged bone and then begins laying down new bone onto the implant surface. In a healthy person, primary stability gradually decreases as the bone remodels, while secondary stability quickly increases and takes over. In a person with osteoporosis, this balance is delicate. The bone’s healing capacity is reduced. The bone-forming cells (osteoblasts) are less active, while the bone-resorbing cells (osteoclasts) may be overactive. The risk is that primary stability wanes before sufficient secondary stability forms, causing the implant to lose its anchor during the critical first 3 to 6 months of healing.
What the Research Tells Us: An Honest Look at the Numbers
For decades, clinicians were cautious. Today, systematic reviews and long-term studies paint a more encouraging, though carefully worded, picture.
- Implant survival rates in osteoporotic patients often fall within an acceptable range, frequently cited between 88% and 95% over a 10-year period, compared to over 95% in healthy individuals. While this difference is statistically significant, it is not a catastrophic gap for the vast majority of patients.
- The quality of evidence is crucial. Many successful studies focus on well-controlled patients whose osteoporosis is managed with medication. Untreated, severe osteoporosis presents a higher and less predictable risk.
- The jawbone location matters enormously. The dense lower front jaw has a consistently high success rate, while the soft, spongy bone in the upper back jaw (posterior maxilla) is the most challenging site for any implant placement and carries a notably higher risk for osteoporotic patients.
- Bone quality, not just density, is key. The micro-architecture of bone—how the tiny struts and plates are connected—plays a massive role. A patient with moderately low density but well-connected bone structure may heal better than a patient with a slightly higher density but disconnected, rod-like bone structure.
Here is a realistic summary table of survival rates, based on a compilation of current clinical literature.
| Jaw Site | Average 5-10 Year Survival in Healthy Patients | Average 5-10 Year Survival in Managed Osteoporotic Patients | Key Clinical Consideration |
|---|---|---|---|
| Anterior Mandible (Lower Front) | 97-99% | 95-97% | The safest zone; dense cortical bone provides excellent primary stability. |
| Posterior Mandible (Lower Back) | 95-98% | 90-95% | Good success, but caution is needed near the nerve canal. |
| Anterior Maxilla (Upper Front) | 96-98% | 92-96% | Aesthetic zone; bone is softer than the lower jaw but success remains high. |
| Posterior Maxilla (Upper Back) | 92-95% | 85-92% | The highest risk zone. Bone is naturally very soft and porous, and sinus proximity adds complexity. |
These numbers are not meant to scare you. They are a tool for a realistic conversation with your surgeon. A 90% success rate means 9 out of 10 implants are still functioning well after many years. That is a strong vote of confidence, but it also acknowledges that the journey demands precise technique and careful maintenance.
Before the Implant: The Medication Conversation
When you discuss osteoporosis and dental implants, you cannot ignore the medications. This is arguably the most critical safety topic in the entire field. The conversation must start not with the implant, but with your drug history. A particular class of medication fundamentally changes the risk profile, and you must be your own best advocate.
The Critical Distinction: Antiresorptives vs. Anabolics
Osteoporosis medications fall into two broad camps: those that slow bone breakdown (antiresorptives) and those that build new bone (anabolics). The antiresorptives are where our major concern lies.
- Bisphosphonates (e.g., Alendronate/Fosamax, Risedronate/Actonel, Zoledronic Acid/Reclast): These are the most common oral and IV medications. They work by sticking to bone and poisoning the osteoclasts, the cells that resorb bone. This slows bone loss effectively, but it also profoundly suppresses the bone’s natural remodeling cycle. The jawbone, which has a very high turnover rate, can be heavily affected. The blood supply can diminish, making the bone unable to heal even a minor trauma like a tooth extraction or an implant surgery.
- Denosumab (Prolia): This is an injectable medication that works differently but has a similar antiresorptive effect. It blocks a signal that activates osteoclasts. Its effect on the bone is potent, but unlike bisphosphonates, it does not stay bound to the skeleton for years.
- Anabolic Agents (e.g., Teriparatide/Forteo): These are a hopeful category. They stimulate bone formation. In some studies, Teriparatide has been used in patients with a history of MRONJ or poor healing to actually enhance peri-implant bone regeneration. This is a specialized, off-label use that represents the cutting edge of treatment.
Medication-Related Osteonecrosis of the Jaw (MRONJ)
This is the complication every responsible clinician seeks to avoid. MRONJ is a condition where the jawbone is exposed and begins to die. It can manifest as a non-healing tooth socket after an extraction, exposed bone in the mouth, pain, swelling, and infection. It is a serious, difficult-to-treat condition.
The risk is directly linked to the type of medication, the duration of use, and the nature of the surgery. The risk for a patient taking an oral bisphosphonate for a few years is very low, perhaps around 0.1% for a dental extraction. For a cancer patient on high-dose IV bisphosphonates or denosumab, the risk can be as high as 1-15%. An implant surgery, which involves drilling into the bone, is a higher-risk procedure than a simple extraction.
A Critical Note for Your Safety: Never stop or pause your osteoporosis medication on your own. This decision requires a coordinated conversation between your prescribing physician, your dentist, and your oral surgeon. Abruptly stopping a drug like denosumab can lead to a rapid rebound in bone loss and an increased risk of spinal fractures. The decision for a “drug holiday” (a temporary pause) is a complex medical judgment.
The Candidacy Evaluation: A Deep-Dive into Your Health
You are not a single scan, and you are certainly not a single diagnosis. Determining if you are a candidate for dental implants is a multi-step detective process. A responsible implantologist will act like a cautious pilot, going through every item on a pre-flight checklist before we ever leave the ground.
The 3D Cone Beam CT Scan: A Non-Negotiable Step
If you have osteoporosis, a standard 2D dental X-ray is entirely insufficient. A Cone Beam Computed Tomography (CBCT) scan is mandatory. This technology creates a 3D model of your jaws, allowing the surgeon to virtually fly through the bone.
With a CBCT, we can:
- Measure the bone’s width and height with sub-millimeter accuracy.
- Visualize the location of vital structures like the inferior alveolar nerve in the lower jaw and the maxillary sinus in the upper jaw.
- Assess bone density in Hounsfield Units (HU). This is a quantitative scale of radiodensity. Dense cortical bone might measure over 1000 HU. Soft, fatty marrow might be negative. A D3 or D4 bone type, common in the posterior maxilla and in osteoporotic patients, will show lower HU values (often 150-350 HU). This gives an objective measure of the biomechanical environment we’re working with.
- Visualize the cortical bone thickness, the hard shell that must grip the implant for primary stability.
A skilled surgeon will use the CBCT to plan the surgery virtually. They will select the exact implant size, angle, and position before you even sit in the chair. This is the gold standard of care.
A Complete Blood Panel: Looking for Hidden Speed Bumps
Osteoporosis doesn’t exist in a vacuum. A thorough blood test is a window into your metabolic state. We are looking for conditions that can mimic or worsen osteoporosis and impair healing. A foundational panel includes:
- Vitamin D3 (25-hydroxyvitamin D): This is non-negotiable. Vitamin D is critical for calcium absorption and bone mineralization. A low level (below 30 ng/ml) is strongly linked to early implant failure. We look for a level sufficient to support healing, typically above 50 ng/ml.
- Complete Blood Count (CBC) and Comprehensive Metabolic Panel (CMP): This screens for anemia, infection, liver and kidney function, and electrolyte balance. Healing demands a massive amount of metabolic work.
- Thyroid Panel (TSH, Free T3, Free T4): Undiagnosed or poorly managed hyperthyroidism is a major cause of secondary osteoporosis and bone loss.
- Sex Hormones (Estradiol, Testosterone): Declining hormone levels drive bone loss in both women and men.
- Bone Turnover Markers (C-Telopeptide/CTX): This is a specific blood test that measures the rate of bone breakdown. A very low CTX result (often below 150 pg/ml) in a patient on antiresorptive drugs signals a heavily suppressed bone metabolism and a high risk of MRONJ. It serves as a guide for risk stratification.
Lifestyle Factors You Can Control
This is the part of the evaluation where you hold immense power. The surgery is a single day, but the healing environment is built over weeks and months beforehand.
- Smoking: This is a direct threat. Nicotine is a potent vasoconstrictor. It chokes off the tiny blood vessels that carry oxygen and healing cells to the surgical site. An osteoporotic bone already has a compromised healing capacity. Smoking amplifies the risk of failure dramatically. A cessation period of at least 4 weeks before and 8 weeks after surgery is a common, and wise, requirement.
- Uncontrolled Diabetes: High blood sugar creates a perfect storm for infection and impairs the function of osteoblasts. An HbA1c test, showing your average blood sugar over three months, gives a clear picture. A level below 7% is a good target for elective surgery.
- Alcohol Intake: Chronic heavy drinking is toxic to bone cells and can impair clotting and healing. Honesty with your surgeon here is crucial.
Adapting the Procedure: How Surgeons Mitigate the Risk
Once you’ve been cleared as a candidate, the surgical protocol itself shifts to one of minimal trauma and maximum precision. The “conventional” technique taught decades ago is not the approach for a patient with compromised bone. Modern implantology has a specific, adapted playbook.
The Atraumatic Surgical Technique
The goal is to preserve every single living bone cell. We avoid overheating the bone, as a temperature above 47°C (117°F) for just one minute can cause permanent bone cell death. The protocol involves:
- Using a sharp, new drill for every surgery.
- Drilling at a very slow speed with copious, chilled saline irrigation.
- Employing a technique called “under-preparation.” This means the final hole drilled in the bone is slightly smaller in diameter than the implant itself. When the implant is screwed in, it compresses the softer bone laterally, increasing its density at the interface. This dramatically improves primary stability in soft bone. This is called bone condensing or osteotome technique.
Choosing the Right Implant: Surface and Design
Not all implants are created equal. For osteoporotic bone, the implant’s features are engineered to compensate for biological shortcomings.
- Surface Technology: Modern implants have a moderately rough, micro-textured surface, created through sandblasting and acid-etching. This surface topography dramatically increases the surface area for bone cells to attach to and accelerates the osseointegration process. Some newer surfaces are even hydrophilic, meaning they attract blood and proteins, further boosting the early healing cascade.
- Implant Macrostructure: The thread design matters. In soft bone, a thread pattern that is deeper, with a sharp cutting edge, helps the implant achieve a strong mechanical bite. Tapered implant bodies act like a wedge, condensing the bone as they are inserted, which provides immediate, high primary stability even in low-density bone.
The Crucial Role of the Healing Timeline
Patience is your most powerful ally. The standard protocol, which may heal in 3-4 months in a healthy patient, is often extended for someone with osteoporosis.
| Healing Phase | Healthy Bone Protocol (Typical) | Osteoporotic Bone Protocol (Recommended) | The Rationale |
|---|---|---|---|
| Implant Uncovering | 3-4 months after placement | 5-8 months after placement | Allowing an extended period of undisturbed osseointegration for the weaker, slower bone remodeling process. |
| Progressive Loading | Immediate or early (6-8 weeks) | Always delayed | A gradual introduction of force. A temporary crown is slowly adjusted to increase the bite pressure over weeks, preventing micro-fractures at the healing bone-implant interface. |
| Final Restoration | Directly after uncovering | After a trial period with a provisional | Confirming the soft tissue and bone have matured into a stable, sustainable architecture around the implant before fabricating the final, permanent crown. |
The surgeon will often use a two-stage approach. The implant is placed and then completely buried under the gum tissue for the entire extended healing period. It is protected from the forces of chewing and the bacteria in the mouth. Only after a successful healing confirmation is it surgically uncovered and a healing abutment placed.
When the Foundation is Weak: The Magic of Bone Grafting
What if the 3D scan reveals that the bone is simply too thin, too short, or too soft for a predictable implant outcome? This is not the end of the road. It is a detour that requires another layer of restorative work: bone grafting. This is the process of adding bone volume and density to create a solid foundation.
A Patient’s Guide to Graft Materials
Your own bone is still the gold standard, but modern science offers excellent alternatives. The choice is a strategic one made by your surgeon.
- Autograft (Your Own Bone): This is bone harvested from another site in your own body, like the chin, the back of the lower jaw, or the hip. It is the only graft that is “alive,” containing your own bone-forming cells and growth factors. It heals by osteogenesis, directly making new bone. The trade-off is a second surgical site and the associated discomfort.
- Allograft (Donor Bone): This is human bone from a certified tissue bank. It is meticulously processed and sterilized. It provides a perfect mineral scaffold for your own cells to grow into. It is conductive, meaning it guides your body’s healing, but not inductive.
- Xenograft (Animal Bone): The most common is bovine (cow) bone. It has a structure very similar to human bone. It is processed to be completely safe and is highly effective. It resorbs very slowly, providing long-term space maintenance as your own bone slowly replaces it.
- Alloplast (Synthetic): These are lab-made, often from calcium phosphate or bioactive glasses. They are designed to be chemically similar to natural bone mineral and are engineered to resorb at a specific rate.
Major Grafting Procedures: Solving Big Problems
- Sinus Lift (Sinus Augmentation): This is the classic solution for the soft, upper back jaw. The floor of the maxillary sinus, an air-filled cavity above your teeth, is gently lifted, and bone graft material is packed into the space created. After a healing period of 6 to 12 months, this new vertical bone can host an implant. It is one of the most predictable and well-studied procedures in implantology, with high success rates even in osteoporotic patients.
- Ridge Augmentation: If the bone ridge is too thin horizontally, a block of bone graft (often an autograft or a mix of materials) is fixed to the side of the jaw with tiny screws. A protective membrane is placed over it, and the gum is closed. This builds out the width of the ridge so an implant can be surrounded 360 degrees by bone.
- Socket Preservation: When a tooth is extracted, the empty socket is immediately packed with a bone graft. This simple, proactive step prevents the inevitable collapse and shrinkage of the bone that follows an extraction. It is far easier and more effective to preserve existing bone than to rebuild it later.
A Clear Contingency Path: Treatment Decision Flowchart
Making this decision can feel overwhelming. To make the path clearer, here is a practical decision-making flowchart that outlines the thought process a responsible clinical team should follow with you.
- Step 1: Medical History Deep-Dive
- Is the patient on antiresorptive medication (bisphosphonates, denosumab)?
- YES, Low Risk (Oral bisphosphonate < 3 years, no other risks): Proceed with caution. Check CTX levels. Obtain physician clearance. Use strict atraumatic protocol.
- YES, High Risk (IV bisphosphonate, long-term oral, on denosumab): Risk of MRONJ is significant. Dental implants are generally contraindicated. Explore non-invasive tooth replacement.
- NO: Proceed to step 2.
- Is the patient on antiresorptive medication (bisphosphonates, denosumab)?
- Step 2: Metabolic and Lifestyle Assessment
- Check Vitamin D, HbA1c, and smoking status. Are they optimized?
- NO: Patient is not an ideal surgical candidate yet. Prescribe a healing protocol: supplement with Vitamin D, manage blood sugar, mandate smoking cessation. Re-evaluate in 6-12 weeks.
- YES: Proceed to step 3.
- Check Vitamin D, HbA1c, and smoking status. Are they optimized?
- Step 3: 3D Bone Volume & Density Scan (CBCT)
- Is there sufficient native bone (height >10mm, width >6mm, HU >250) for primary stability?
- YES: Proceed to implant surgery with an adapted, extended healing protocol.
- NO, but correctable: Proceed to step 4. Plan a bone grafting procedure (Sinus lift, ridge augmentation) before or during implant placement. Healing time will double.
- NO, and not correctable: The anatomical deficit is too severe (e.g., nerve position, massive bone loss). Implants are not recommended. Discuss removable prosthetics.
- Is there sufficient native bone (height >10mm, width >6mm, HU >250) for primary stability?
The Daily Practice: Post-Operative Care and Lifelong Maintenance
The moment the surgery is complete, the spotlight shifts from the surgeon’s hands to your daily habits. For a patient with osteoporosis, post-operative care is not just about comfort; it is a proactive defense against failure.
The Immediate Healing Phase: First 3 Months
Your surgeon will give you strict instructions. Following them is a critical part of the treatment.
- Nutrition as Medicine: Your body needs raw materials to build bone. Focus on a diet rich in calcium (leafy greens, dairy, fortified alternatives) and high-quality protein. Avoid hard, crunchy, or chewy foods that can transmit micro-movement to the healing implant. Soft, nutrient-dense foods are your best friend.
- Oral Hygiene as a Ritual: In the first days, you may not brush the site directly. You will rinse gently with a prescribed chlorhexidine mouthwash or warm salt water. As healing progresses, an ultra-soft toothbrush becomes your primary tool. The goal is to keep the area totally free of plaque, the sticky film of bacteria that causes inflammation.
- Strictly No Smoking: This cannot be said enough. Smoking during the healing phase is one of the most reliable predictors of implant failure.
The Long Game: Peri-Implantitis and Your Role in Prevention
The long-term enemy of a dental implant is not osteoporosis itself, but a disease called peri-implantitis. This is an infection-induced inflammation that destroys the bone and gum around an integrated implant. Think of it as deep gum disease for an implant. A patient with osteoporosis is potentially more vulnerable because the bone’s natural defense and remodeling capacity are already reduced.
Your defense strategy is a three-legged stool:
- Impeccable Home Care: Brushing twice daily, using an interdental brush or a water flosser to clean around the implant crown, and using non-abrasive toothpaste.
- Professional Maintenance: You are no longer a “twice-a-year” patient. A 3 to 4-month recall schedule with a dental hygienist is non-negotiable. They have specialized non-metal instruments to clean the implant surface without scratching it, a scratch that would harbor bacteria.
- Annual Monitoring: At each visit, the dentist will gently probe around the implant to check gum health and will take a once-a-year X-ray to compare bone levels. A stable, unchanging bone level is the definition of success. Any progressive bone loss is an alarm that requires immediate intervention, often with a deep cleaning of the infected implant surface.
Realistic Alternatives When Implants Are Truly Not an Option
There is a profound peace that comes from accepting the right path, even if it wasn’t your first choice. If your medical and anatomical evaluation definitively rules out implants, you still have excellent, life-changing options. A modern, well-made bridge or denture is not a “failure.” It is a brilliant, safe solution.
The High-Quality Removable Overdenture
This is a game-changer for the lower jaw, in particular. Two to four strategically placed implants, often using shorter or narrower designs that require less bone, can snap a denture firmly into place. The denture clicks onto the implants, providing rock-solid stability. There is no embarrassing slip during a conversation. You can chew with confidence. It’s often called a “Snap-On Smile.” For an osteoporotic patient, this often represents the sweet spot of being a minimally-invasive, highly-successful, and life-altering treatment.
The Precision Partial Denture
For replacing a single tooth or a small group of teeth, a lightweight, frame-based partial denture made of chrome cobalt can be an elegant solution. It is removable for cleaning but does not require surgery. The design can be modified to rest on natural teeth with minimal stress, preserving the remaining dentition.
The Resin-Bonded Bridge (Maryland Bridge)
For replacing a single front tooth, this is a minimally-invasive option. A porcelain tooth is fused to thin metal or ceramic “wings.” These wings are bonded to the back of the adjacent, healthy teeth. It requires almost no drilling on the neighboring teeth, unlike a traditional bridge. It’s a beautiful, conservative, and lower-cost option when a single implant is deemed too risky.
FAQ: Your Questions Answered Directly
Can I get dental implants if I have severe osteoporosis?
Severe osteoporosis increases the risk of poor primary stability and failed osseointegration. It is not an absolute no, but it demands a very critical evaluation. Your candidacy will depend on the jawbone’s specific quality on a 3D scan and your overall health. The risk of failure is significantly higher than in a healthy patient.
What is the safest osteoporosis medication to be on for implant surgery?
The safest situation is being on an anabolic agent like teriparatide, which may actually help bone healing. Among the antiresorptives, a short-term course of an oral bisphosphonate carries a much lower MRONJ risk than a long-term, high-dose IV regimen. However, safety is relative. Any medication decision must involve your physician and surgeon in a shared risk assessment.
My doctor suggested a “drug holiday” before my implant. Is this safe?
A drug holiday can be a risk-reduction strategy for some patients on long-term bisphosphonates, allowing some bone turnover to resume. It is a highly individualized decision. It may be dangerous for a patient with a high spinal fracture risk. This strategy is generally not effective for denosumab, as its effect wears off differently. Your physician must direct this decision.
How much longer does healing take for a patient with osteoporosis?
You should expect and plan for a healing phase that is 1.5 to 2 times longer than the standard protocol. Where a healthy patient might receive a final crown in 4 months, your timeline could easily be 6 to 9 months. A delayed, progressive loading protocol is a mark of a careful, responsible clinician, not an indication of a problem.
Is a same-day implant and crown possible with osteoporosis?
This concept, called immediate loading, is a very high-risk protocol for an osteoporotic patient. The forces of immediate chewing on an unintegrated implant in soft bone are a recipe for micro-motion and failure. Avoid any clinician who promises a same-day fixed tooth in your case without a profoundly careful justification and a recognized, published protocol for it.
What is the single most important thing I can do to ensure my implant lasts?
After the skill of the surgeon, the most important factor is your long-term, at-home hygiene and your commitment to strict professional maintenance every 3-4 months. Preventing peri-implantitis is the key to a lifetime of service from your implant.
Additional Resource: The Link to BoneScience
For further, reputable reading, the American Academy of Implant Dentistry (AAID) and the International Osteoporosis Foundation (IOF) provide patient resources. A direct link to the AAID’s patient information page can be found by searching “AAID patient resources dental implants” in your preferred search engine.
In Conclusion: A Balanced Path Forward
Osteoporosis changes the landscape of dental implant treatment, requiring a meticulous, cautious, and deeply personalized approach, but it does not universally close the door. The journey to a restored smile hinges on a rigorous pre-surgical evaluation, a perfectly adapted surgical technique, and an extended, patient healing period that honors your body’s slower timeline. Ultimately, the path you choose must be a shared decision between you, your physician, and a skilled surgical team, where safety and long-term biological stability are valued above speed or simplicity.
Disclaimer: This article is for informational purposes only and does not constitute medical or dental advice. The content is not intended to be a substitute for professional diagnosis, treatment, or guidance. Always seek the advice of your physician, dentist, or another qualified health provider with any questions you may have regarding a medical or dental condition. Never disregard professional advice or delay in seeking it because of something you have read in this article.